

Carbapenem-Resistant Enterobacteriaceae in Children, United States, 1999-2012
- PMID: 26486124
- PMCID: PMC4622248
- DOI: 10.3201/eid2111.150548
Carbapenem-Resistant Enterobacteriaceae in Children, United States, 1999-2012
Abstract
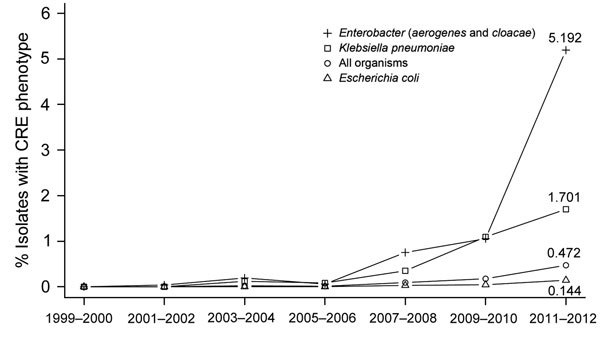
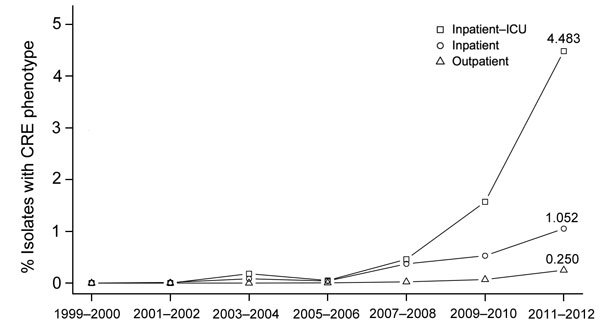
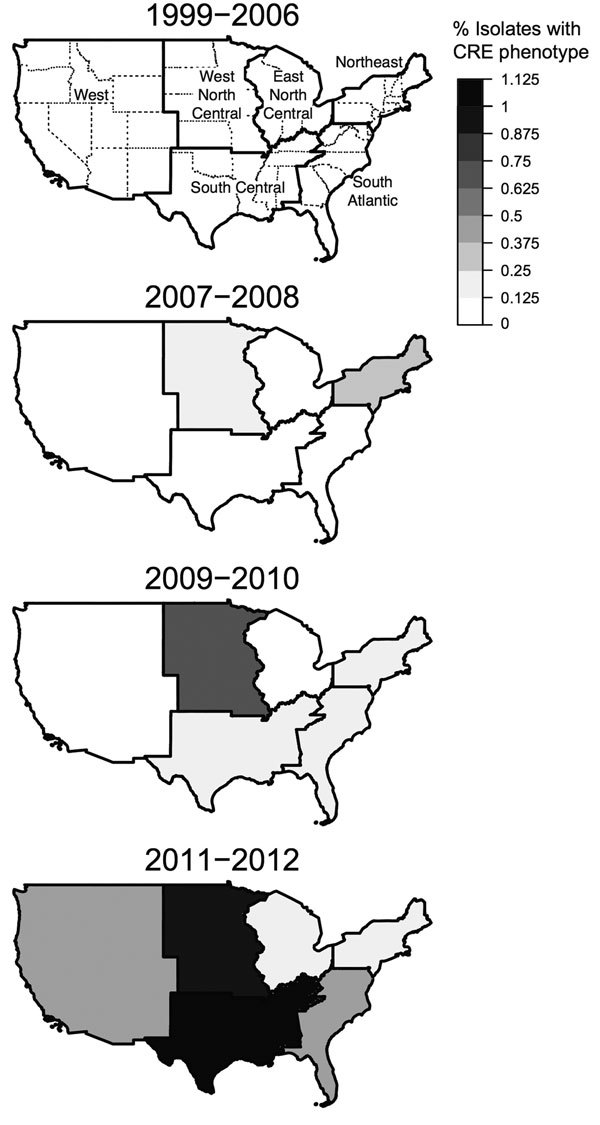
The prevalence of carbapenem-resistant Enterobacteriaceae (CRE) infections is increasing in the United States. However, few studies have addressed their epidemiology in children. To phenotypically identify CRE isolates cultured from patients 1-17 years of age, we used antimicrobial susceptibilities of Enterobacteriaceae reported to 300 laboratories participating in The Surveillance Network-USA database during January 1999-July 2012. Of 316,253 isolates analyzed, 266 (0.08%) were identified as CRE. CRE infection rate increases were highest for Enterobacter species, blood culture isolates, and isolates from intensive care units, increasing from 0.0% in 1999-2000 to 5.2%, 4.5%, and 3.2%, respectively, in 2011-2012. CRE occurrence in children is increasing but remains low and is less common than that for extended-spectrum β-lactamase-producing Enterobacteriaceae. The molecular characterization of CRE isolates from children and clinical epidemiology of infection are essential for development of effective prevention strategies.
Keywords: CRE; Surveillance Network–USA database; United States; antibacterial agents; antimicrobial resistance; bacteria; carbapenem-resistant Enterobacteriaceae; children; epidemiology; infections; β-lactamases.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
