

Topical management of striae distensae (stretch marks): prevention and therapy of striae rubrae and albae
- PMID: 26486318
- PMCID: PMC5057295
- DOI: 10.1111/jdv.13223
Topical management of striae distensae (stretch marks): prevention and therapy of striae rubrae and albae
Abstract
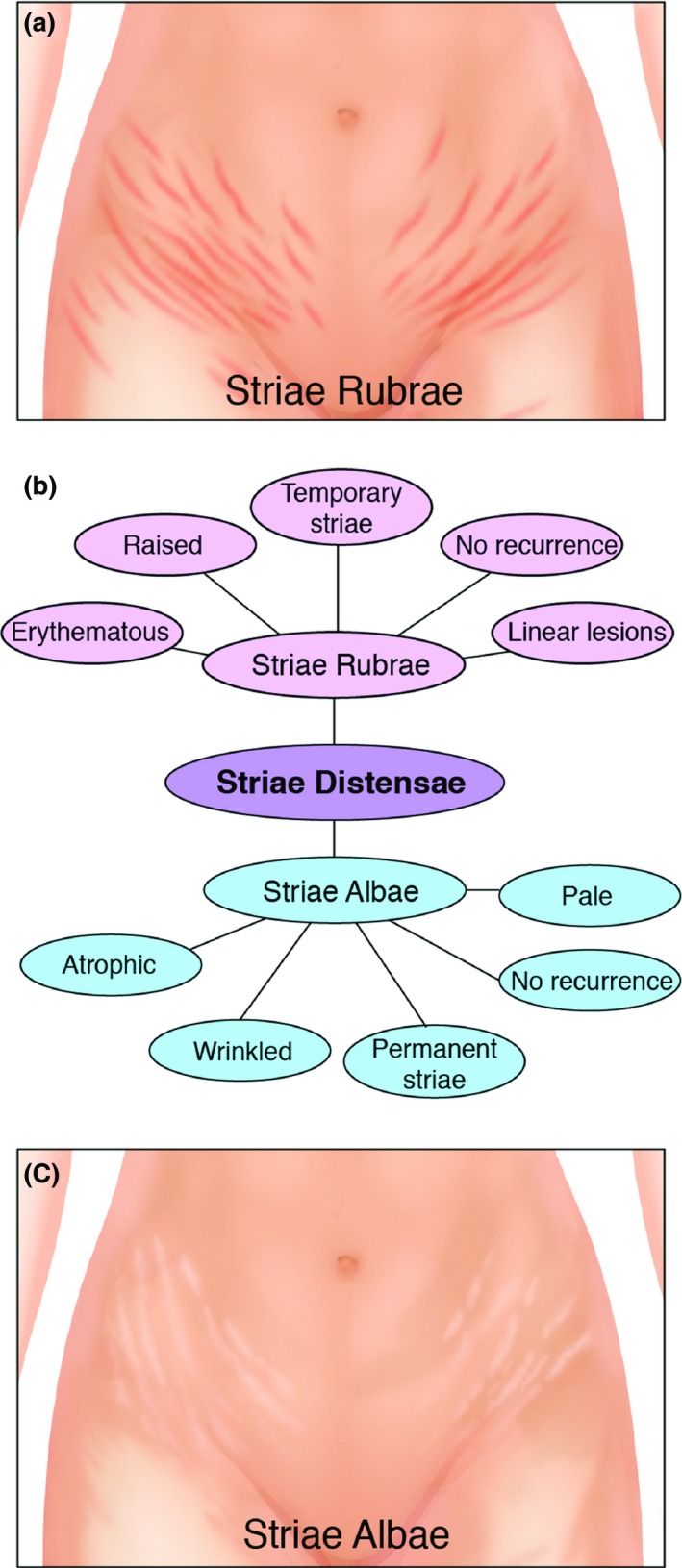
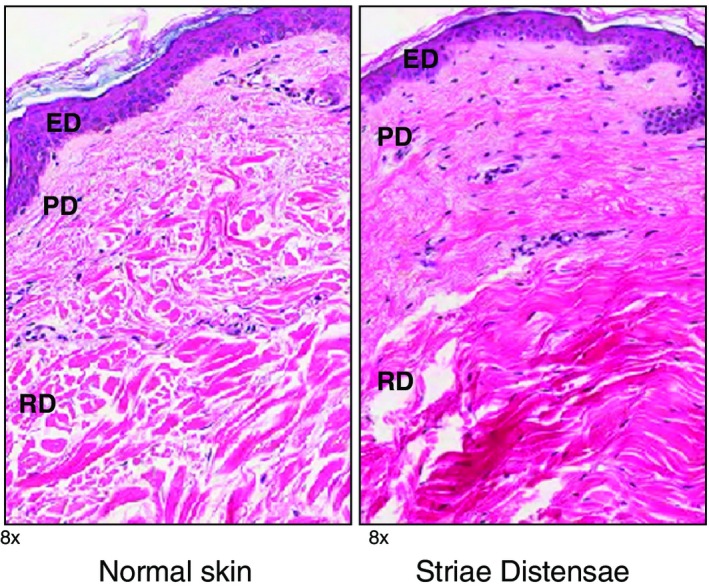
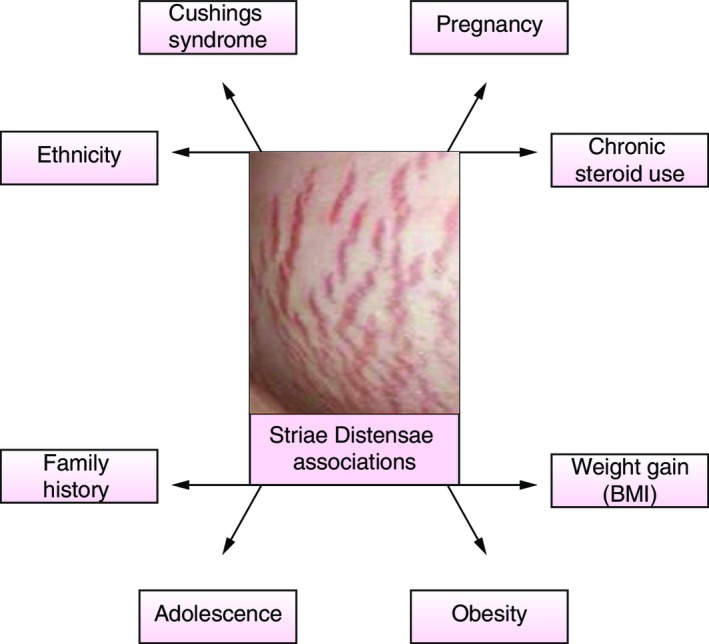
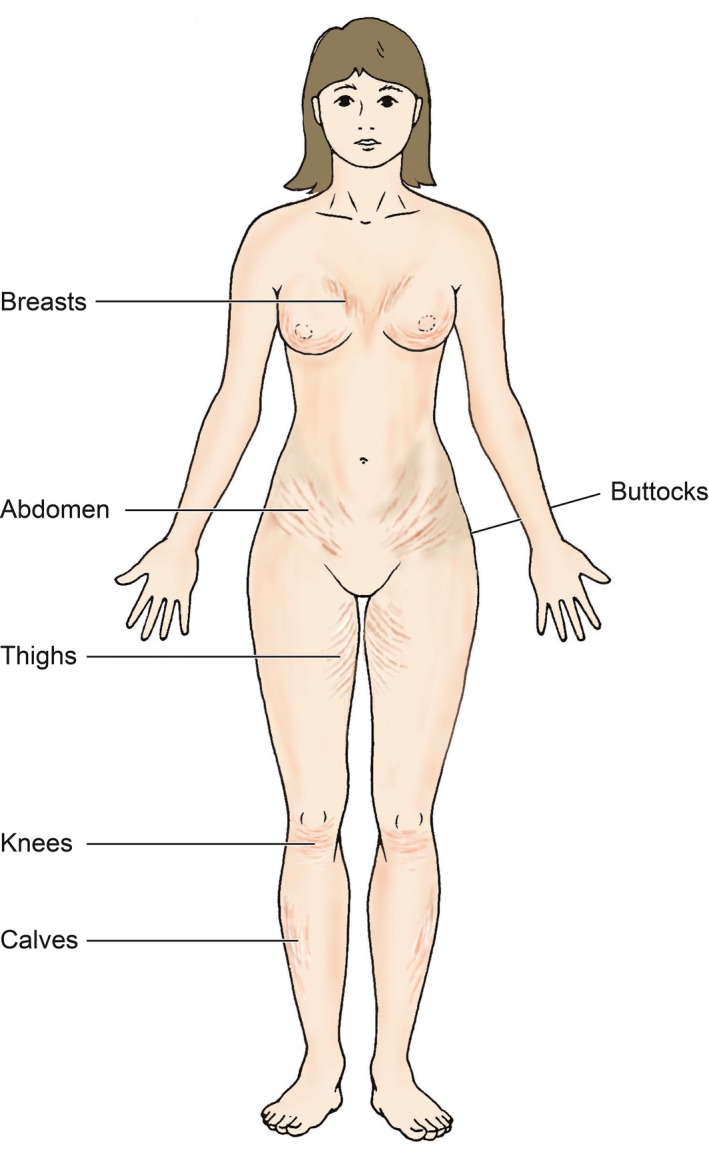
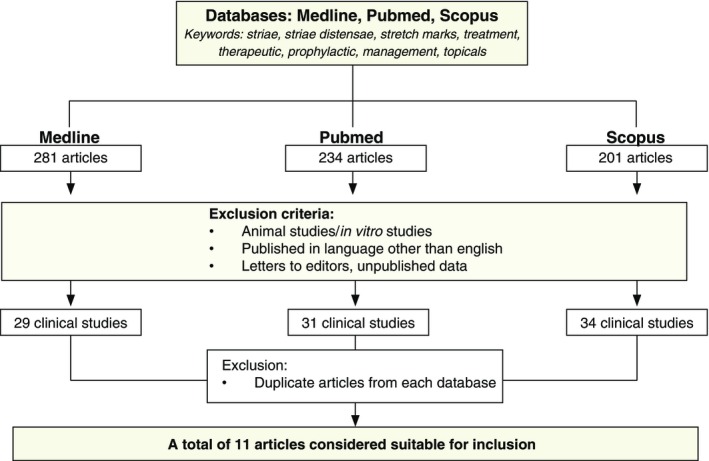
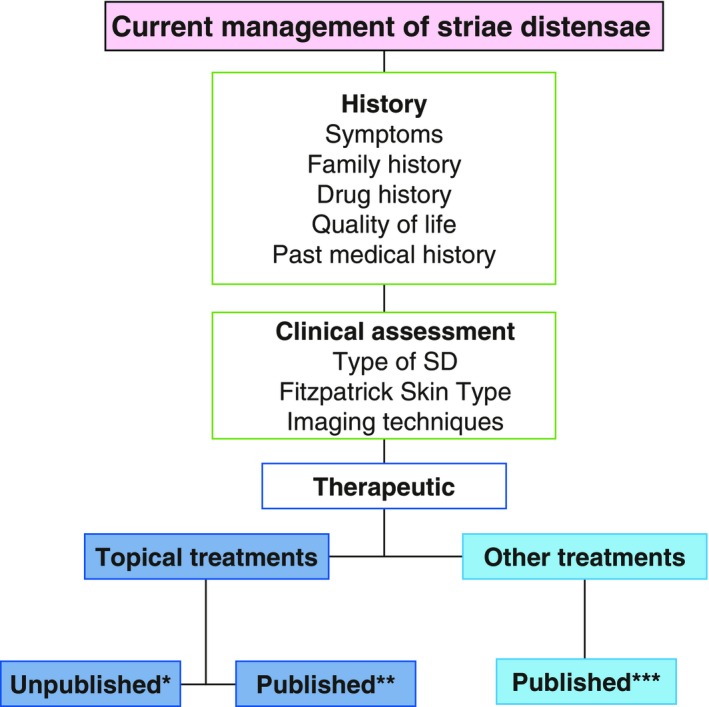
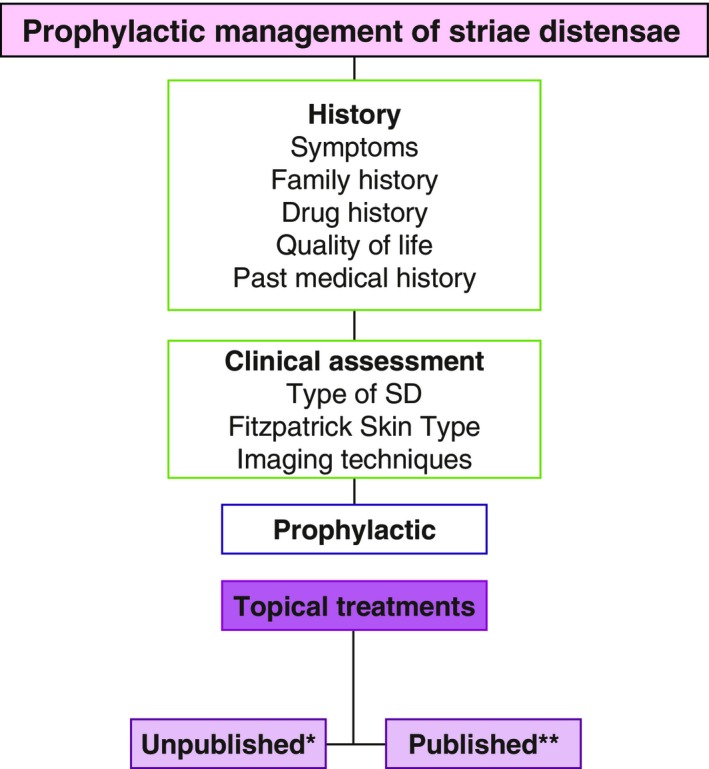
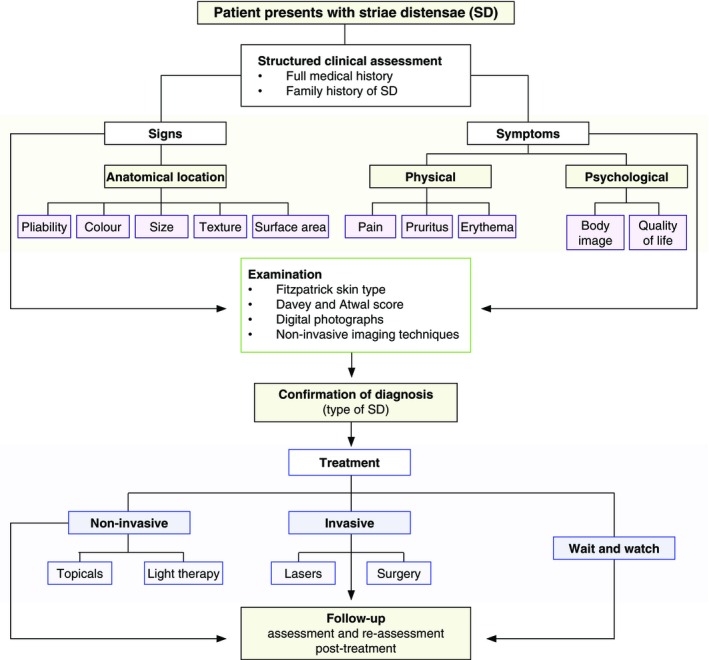
Striae distensae (SD) are common dermal lesions, with significant physical and psychological impact. Many therapeutic modalities are available but none can completely eradicate SD. The most common therapy is the application of topicals used both therapeutically and prophylactically. Even though there are many commercially available topical products, not all have sufficient level of evidence to support their continued use in SD. The aim here was to assess the evidence for the use of topicals in SD and to propose a structured approach in managing SD. A systematic search of published literature and manufacturer website information for topicals in SD was carried out. The results showed that there are few studies (n = 11) which investigate the efficacy of topicals in management of SD. Trofolastin and Alphastria creams demonstrated level-2 evidence of positive results for their prophylactic use in SD. Additionally, tretinoin used therapeutically showed varying results whilst cocoa butter and olive oil did not demonstrate any effect. Overall, there is a distinct lack of evidence for each topical formulation. The majority of topicals failed to mention their effect on early vs. later stages of SD (striae rubrae compared to striae albae) and their role in both prevention and treatment. In conclusion, there is no topical formulation, which is shown to be most effective in eradicating or improving SD. A structured approach in identification and targeted management of symptoms and signs with the appropriate topical is required. Randomized controlled trials are necessary to assess the efficacy of topical products for treatment and prevention of different stages of SD.
© 2015 The Authors. Journal of the European Academy of Dermatology and Venereology published by John Wiley & Sons Ltd on behalf of European Academy of Dermatology and Venereology.
Figures
References
-
- de Angelis F, Kolesnikova L, Renato F, Liguori G. Fractional nonablative 1540‐nm laser treatment of striae distensae in Fitzpatrick skin types II to IV: clinical and histological results. Aesthet Surg J 2011; 31: 411–419. - PubMed
-
- Elson ML. Topical tretinoin in the treatment of striae distensae and in the promotion of wound healing: a review. J Dermatol Treat 1994; 5: 163–165.
-
- Kang S. Topical tretinoin therapy for management of early striae. J Am Acad Dermatol 1998; 39: S90–S92. - PubMed
-
- Kim BJ, Lee DH, Kim MN et al Fractional photothermolysis for the treatment of striae distensae in Asian skin. Am J Clin Dermatol 2008; 9: 33–37. - PubMed
-
- Sheu HM, Yu HS, Chang CH. Mast cell degranulation and elastolysis in the early stage of striae distensae. J Cutan Pathol 1991; 18: 410–416. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
