

A pilot cohort study of cerebral autoregulation and 2-year neurodevelopmental outcomes in neonates with hypoxic-ischemic encephalopathy who received therapeutic hypothermia
- PMID: 26486728
- PMCID: PMC4618147
- DOI: 10.1186/s12883-015-0464-4
A pilot cohort study of cerebral autoregulation and 2-year neurodevelopmental outcomes in neonates with hypoxic-ischemic encephalopathy who received therapeutic hypothermia
Abstract
Background: Neurodevelopmental disabilities persist in survivors of neonatal hypoxic-ischemic encephalopathy (HIE) despite treatment with therapeutic hypothermia. Cerebrovascular autoregulation, the mechanism that maintains cerebral perfusion during changes in blood pressure, may influence outcomes. Our objective was to describe the relationship between acute autoregulatory vasoreactivity during treatment and neurodevelopmental outcomes at 2 years of age.
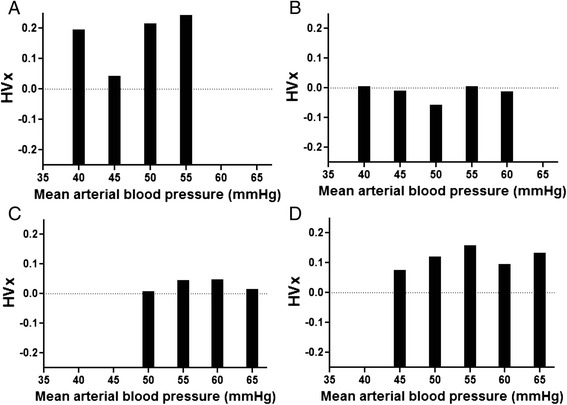
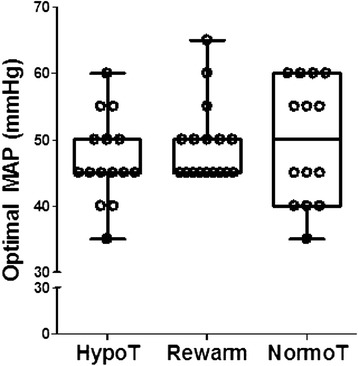
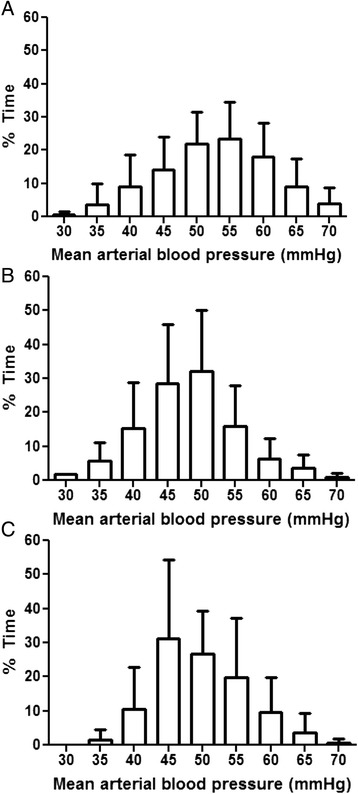
Methods: In a pilot study of 28 neonates with HIE, we measured cerebral autoregulatory vasoreactivity with the hemoglobin volume index (HVx) during therapeutic hypothermia, rewarming, and the first 6 h of normothermia. The HVx, which is derived from near-infrared spectroscopy, was used to identify the individual optimal mean arterial blood pressure (MAPOPT) at which autoregulatory vasoreactivity is greatest. Cognitive and motor neurodevelopmental evaluations were completed in 19 children at 21-32 months of age. MAPOPT, blood pressure in relation to MAPOPT, blood pressure below gestational age + 5 (ga + 5), and regional cerebral oximetry (rSO2) were compared to the neurodevelopmental outcomes.
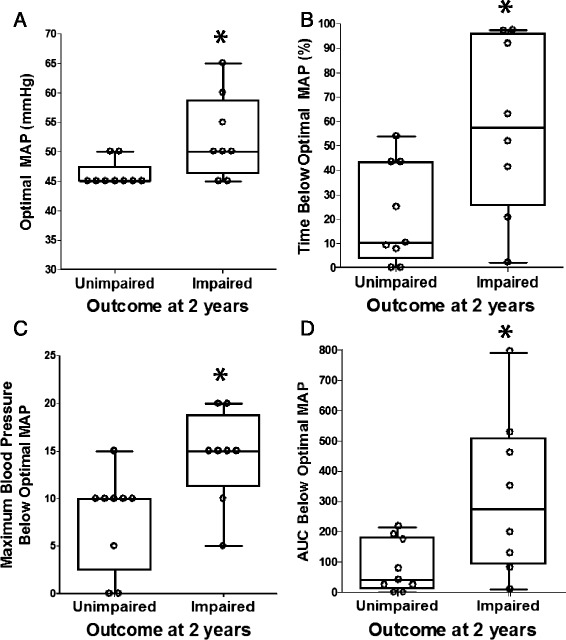
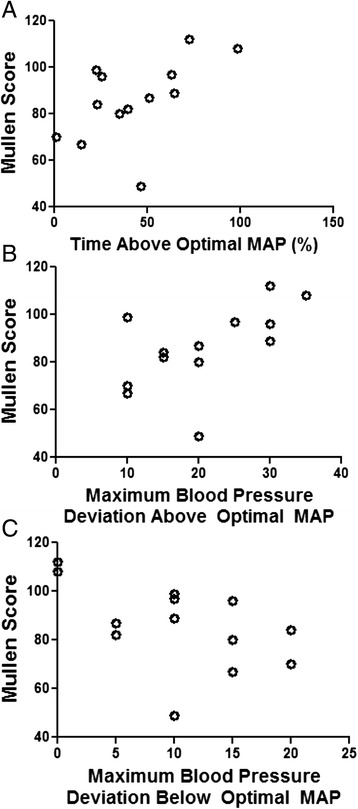
Results: Nineteen children who had HIE and were treated with therapeutic hypothermia performed in the average range on cognitive and motor evaluations at 21-32 months of age, although the mean performance was lower than that of published normative samples. Children with impairments at the 2-year evaluation had higher MAPOPT values, spent more time with blood pressure below MAPOPT, and had greater blood pressure deviation below MAPOPT during rewarming in the neonatal period than those without impairments. Greater blood pressure deviation above MAPOPT during rewarming was associated with less disability and higher cognitive scores. No association was observed between rSO2 or blood pressure below ga + 5 and neurodevelopmental outcomes.
Conclusion: In this pilot cohort, motor and cognitive impairments at 21-32 months of age were associated with greater blood pressure deviation below MAPOPT during rewarming following therapeutic hypothermia, but not with rSO2 or blood pressure below ga + 5. This suggests that identifying individual neonates' MAPOPT is superior to using hemodynamic goals based on gestational age or rSO2 in the acute management of neonatal HIE.
Figures

References
-
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Munson ML. Births: final data for 2003. Natl Vital Stat Rep. 2005;54(2):1–116. - PubMed
-
- US Department of Health and Human Services Centers for Disease Control and Prevention. Economic costs associated with mental retardation, cerebral palsy, hearing loss, and vision impairment – United States, 2003. MMWR Morb Mortality Wkly Rep. 2004;53(03):57–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
