

A randomized controlled behavioral intervention trial to improve medication adherence in adult stroke patients with prescription tailored Short Messaging Service (SMS)-SMS4Stroke study
- PMID: 26486857
- PMCID: PMC4618367
- DOI: 10.1186/s12883-015-0471-5
A randomized controlled behavioral intervention trial to improve medication adherence in adult stroke patients with prescription tailored Short Messaging Service (SMS)-SMS4Stroke study
Abstract
Background: The effectiveness of mobile technology to improve medication adherence via customized Short Messaging Service (SMS) reminders for stroke has not been tested in resource poor areas. We designed a randomized controlled trial to test the effectiveness of SMS on improving medication adherence in stroke survivors in Pakistan.
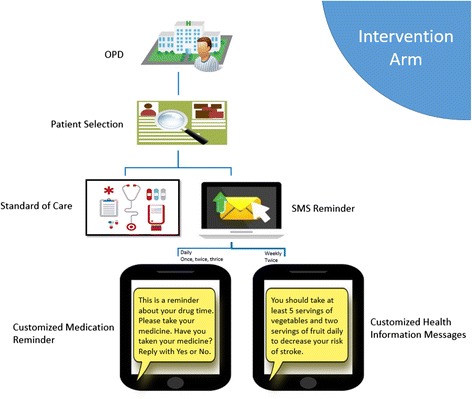
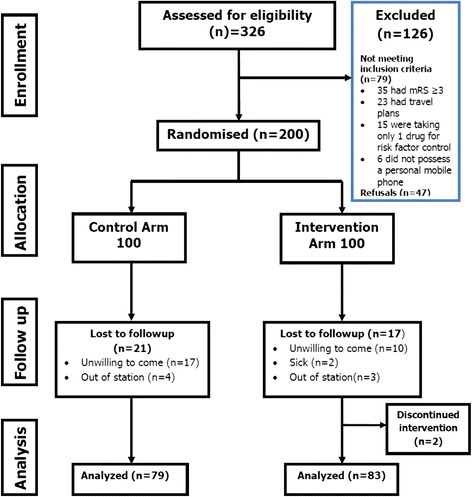
Methods: This was a parallel group, assessor-blinded, randomized, controlled, superiority trial. Participants were centrally randomized in fixed block sizes. Adult participants on multiple medications with access to a cell phone and stroke at least 4 weeks from onset (Onset as defined by last seen normal) were eligible. The intervention group, in addition to usual care, received reminder SMS for 2 months that contained a) Personalized, prescription tailored daily medication reminder(s) b) Twice weekly health information SMS. The Health Belief Model and Social Cognitive theory were used to design the language and content of messages. Frontline SMS software was used for SMS delivery. Medication adherence was self-reported and measured on the validated Urdu version of Morisky Medication Adherence Questionnaire. Multiple linear regression was used to model the outcome against intervention and other covariates. Analysis was conducted by intention-to-treat principle.
Results: Two hundred participants were enrolled. 38 participants were lost to follow-up. After 2 months, the mean medication score was 7.4 (95 % CI: 7.2-7.6) in the intervention group while 6.7 (95 % CI: 6.4-7.02) in the control group. The adjusted mean difference (Δ) was 0.54 (95 % CI: 0.22-0.85). The mean diastolic blood pressure in the intervention group was 2.6 mmHg (95 % CI; -5.5 to 0.15) lower compared to the usual care group.
Conclusion: A short intervention of customized SMS can improve medication adherence and effect stroke risk factors like diastolic blood pressure in stroke survivors with complex medication regimens living in resource poor areas.
Trial registration: Clinicaltrials.gov NCT01986023 last accessed at https://clinicaltrials.gov/ct2/show/NCT01986023.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2197–223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
-
- Krishnamurthi RV, Feigin VL, Forouzanfar MH, Mensah GA, Connor M, Bennett DA, et al. Global and regional burden of first-ever ischaemic and haemorrhagic stroke during 1990–2010: findings from the global burden of disease study 2010. Lancet Glob Health. 2013;1(5):e259–81. doi: 10.1016/S2214-109X(13)70089-5. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
