

Potential for Drug-Drug Interactions between Antiretrovirals and HCV Direct Acting Antivirals in a Large Cohort of HIV/HCV Coinfected Patients
- PMID: 26488159
- PMCID: PMC4619009
- DOI: 10.1371/journal.pone.0141164
Potential for Drug-Drug Interactions between Antiretrovirals and HCV Direct Acting Antivirals in a Large Cohort of HIV/HCV Coinfected Patients
Abstract
Objectives: Development of direct acting antivirals (DAA) offers new benefits for patients with chronic hepatitis C. The combination of these drugs with antiretroviral treatment (cART) is a real challenge in HIV/HCV coinfected patients. The aim of this study was to describe potential drug-drug interactions between DAAs and antiretroviral drugs in a cohort of HIV/HCV coinfected patients.
Methods: Cross-sectional study of all HIV/HCV coinfected patients attending at least one visit in 2012 in the multicenter French Dat'AIDS cohort. A simulation of drug-drug interactions between antiretroviral treatment and DAAs available in 2015 was performed.
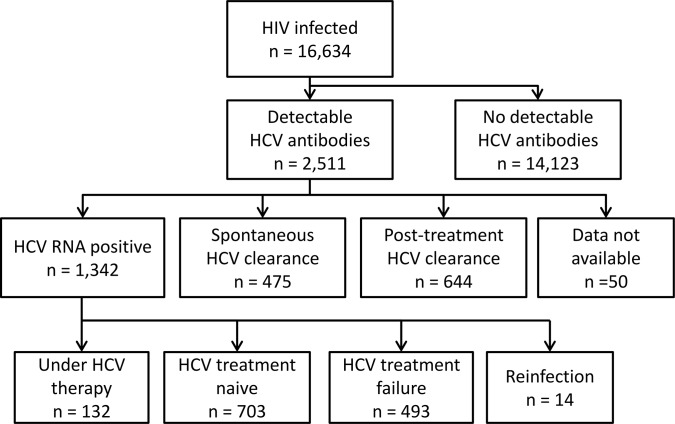
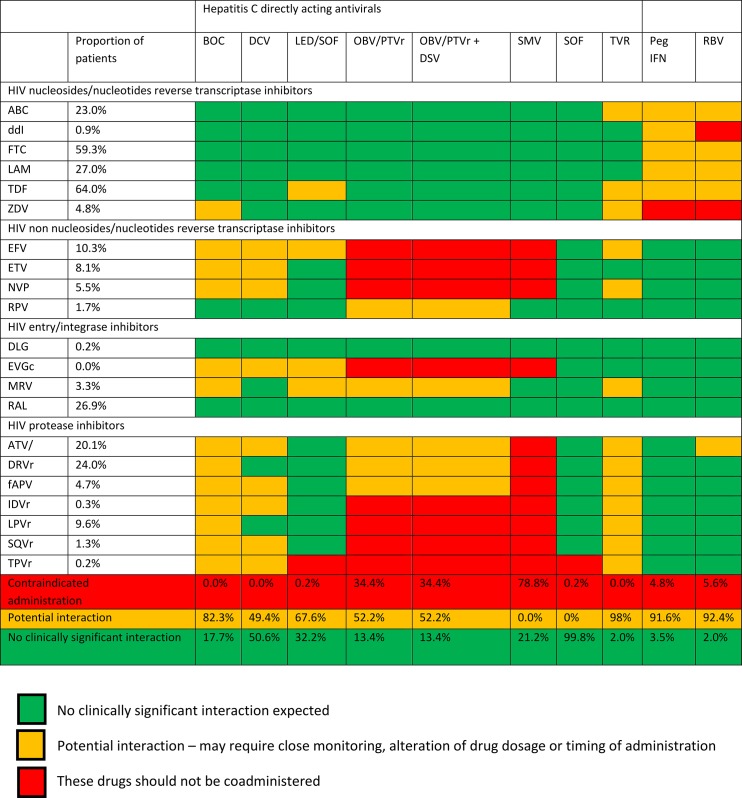
Results: Of 16,634 HIV-infected patients, 2,511 had detectable anti-HCV antibodies, of whom 1,196 had a detectable HCV-RNA and were not receiving HCV treatment at the time of analysis. 97.1% of these patients were receiving cART and 81.2% had a plasma HIV RNA <50 copies/mL. cART included combinations of nucleoside reverse transcriptase inhibitors with a boosted protease inhibitor in 43.6%, a non-nucleoside reverse transcriptase inhibitor in 17.3%, an integrase inhibitor in 15.4% and various combinations or antiretroviral drugs in 23.7% of patients. A previous treatment against HCV had been administered in 64.4% of patients. Contraindicated associations/potential interactions were expected between cART and respectively sofosbuvir (0.2%/0%), sofosbuvir/ledipasvir (0.2%/67.6%), daclatasvir (0%/49.4%), ombitasvir/boosted paritaprevir (with or without dasabuvir) (34.4%/52.2%) and simeprevir (78.8%/0%).
Conclusions: Significant potential drug-drug interactions are expected between cART and the currently available DAAs in the majority of HIV/HCV coinfected patients. Sofosbuvir/ledipasvir and sofosbuvir/daclatasvir with or without ribavirin appeared the most suitable combinations in our population. A close collaboration between hepatologists and HIV/AIDS specialists appears necessary for the management of HCV treatment concomitantly to cART.
Conflict of interest statement
Figures
References
-
- Thein HH, Yi Q, Dore GJ, Krahn MD. Natural history of hepatitis C virus infection in HIV-infected individuals and the impact of HIV in the era of highly active antiretroviral therapy: a meta-analysis. AIDS. 2008;22(15):1979–91. Epub 2008/09/12. 10.1097/QAD.0b013e32830e6d51 00002030-200810010-00010 [pii]. . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
