

Safety and Efficacy of Combined Extracorporeal CO2 Removal and Renal Replacement Therapy in Patients With Acute Respiratory Distress Syndrome and Acute Kidney Injury: The Pulmonary and Renal Support in Acute Respiratory Distress Syndrome Study
- PMID: 26488219
- PMCID: PMC4648187
- DOI: 10.1097/CCM.0000000000001296
Safety and Efficacy of Combined Extracorporeal CO2 Removal and Renal Replacement Therapy in Patients With Acute Respiratory Distress Syndrome and Acute Kidney Injury: The Pulmonary and Renal Support in Acute Respiratory Distress Syndrome Study
Abstract
Objective: To assess the safety and efficacy of combining extracorporeal CO2 removal with continuous renal replacement therapy in patients presenting with acute respiratory distress syndrome and acute kidney injury.
Design: Prospective human observational study.
Settings: Patients received volume-controlled mechanical ventilation according to the acute respiratory distress syndrome net protocol. Continuous venovenous hemofiltration therapy was titrated to maintain maximum blood flow and an effluent flow of 45 mL/kg/h with 33% predilution.
Patients: Eleven patients presenting with both acute respiratory distress syndrome and acute kidney injury required renal replacement therapy.
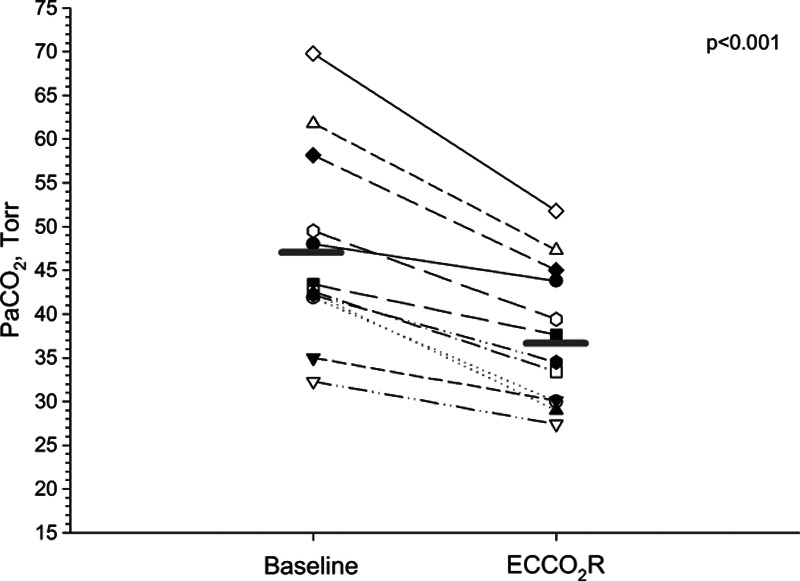
Interventions: A membrane oxygenator (0.65 m) was inserted within the hemofiltration circuit, either upstream (n = 7) or downstream (n = 5) of the hemofilter. Baseline corresponded to tidal volume 6 mL/kg of predicted body weight without extracorporeal CO2 removal. The primary endpoint was 20% reduction in PaCO2 at 20 minutes after extracorporeal CO2 removal initiation. Tidal volume was subsequently reduced to 4 mL/kg for the remaining 72 hours.
Measurements and main results: Twelve combined therapies were conducted in the 11 patients. Age was 70 ± 9 years, Simplified Acute Physiology Score II was 69 ± 13, Sequential Organ Failure Assessment score was 14 ± 4, lung injury score was 3 ± 0.5, and PaO2/FIO2 was 135 ± 41. Adding extracorporeal CO2 removal at tidal volume 6 mL/kg decreased PaCO2 by 21% (95% CI, 17-25%), from 47 ± 11 to 37 ± 8 Torr (p < 0.001). Lowering tidal volume to 4 mL/kg reduced minute ventilation from 7.8 ± 1.5 to 5.2 ± 1.1 L/min and plateau pressure from 25 ± 4 to 21 ± 3 cm H2O and raised PaCO2 from 37 ± 8 to 48 ± 10 Torr (all p < 0.001). On an average of both positions, the oxygenator's blood flow was 410 ± 30 mL/min and the CO2 removal rate was 83 ± 20 mL/min. The oxygenator blood flow (p <0.001) and the CO2 removal rate (p = 0.083) were higher when the membrane oxygenator was placed upstream of the hemofilter. There was no safety concern.
Conclusions: Combining extracorporeal CO2 removal and continuous venovenous hemofiltration in patients with acute respiratory distress syndrome and acute kidney injury is safe and allows efficient blood purification together with enhanced lung protective ventilation.
Conflict of interest statement
Dr. Allardet-Servent’s institution received grant support from ARARD (contribution to the paiement of membrane oxygenator). The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures




Comment in
-
Assessing Feasibility (and Increasing Simplicity) in Extracorporeal Rescue Therapy for Acute Respiratory Distress Syndrome: The Pulmonary and Renal Support in Acute Respiratory Distress Syndrome Study.Crit Care Med. 2015 Dec;43(12):2683-5. doi: 10.1097/CCM.0000000000001364. Crit Care Med. 2015. PMID: 26575659 No abstract available.
References
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–1693. - PubMed
-
- Brun-Buisson C, Minelli C, Bertolini G, et al. ALIVE Study Group. Epidemiology and outcome of acute lung injury in European intensive care units. Results from the ALIVE study. Intensive Care Med. 2004;30:51–61. - PubMed
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342:1334–1349. - PubMed
-
- Rouby JJ, Puybasset L, Nieszkowska A, et al. Acute respiratory distress syndrome: Lessons from computed tomography of the whole lung. Crit Care Med. 2003;31:S285–S295. - PubMed
-
- Gattinoni L, Pesenti A. The concept of “baby lung”. Intensive Care Med. 2005;31:776–784. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
