

Chronic Subdural Hematoma Associated with Spontaneous Intracranial Hypotension: Therapeutic Strategies and Outcomes of 55 Cases
- PMID: 26489406
- PMCID: PMC4756246
- DOI: 10.2176/nmc.oa.2015-0032
Chronic Subdural Hematoma Associated with Spontaneous Intracranial Hypotension: Therapeutic Strategies and Outcomes of 55 Cases
Abstract
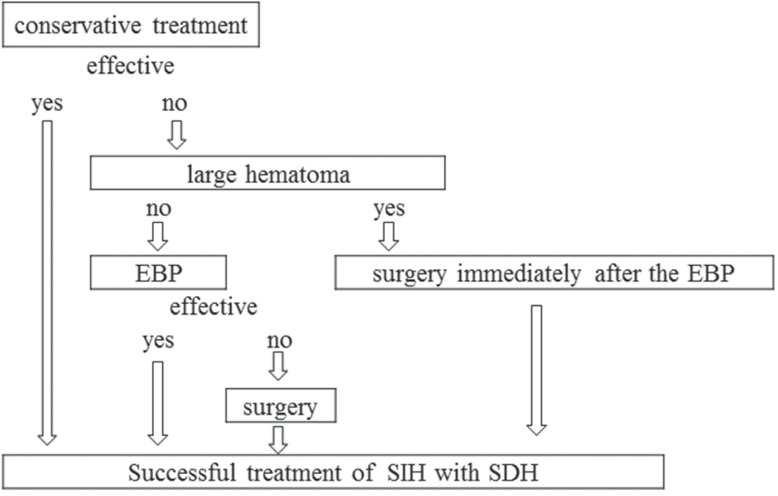
Spontaneous intracranial hypotension (SIH) has increasingly been recognized, and it is well known that SIH is sometimes complicated by chronic subdural hematoma (SDH). In this study, 55 cases of SIH with SDH were retrospectively analyzed, focusing on therapeutic strategies and outcomes. Of 169 SIH cases (75 males, 84 females), 55 (36 males, 19 females) were complicated by SDH. SIH was diagnosed based on clinical symptoms, neuroimaging, and/or low cerebrospinal fluid pressure. Presence of orthostatic headache and diffuse meningeal enhancement on magnetic resonance imaging were regarded as the most important criteria. Among 55 SIH with SDH cases, 13 improved with conservative treatment, 25 initially received an epidural blood patch (EBP), and 17 initially underwent irrigation of the hematomas. Of the 25 initially treated with EBP, 7 (28.0%) needed SDH surgery and 18 (72.0%) recovered fully without surgery. Of 17 SDH cases initially treated with surgery, 6 (35.7%) required no EBP therapy and the other 11 (64.3%) needed EBP and/or additional SDH operations. In the latter group, 2 cases had transient severe complications during and after the procedures. One of these 2 cases developed a hoarse voice complication. Despite this single, non-severe complication, all enrolled in this study achieved good outcomes. The present study suggests that patients initially receiving SDH surgery may need additional treatments and may occasionally have complications. If conservative treatment is insufficient, EBP should be performed prior to hematoma irrigation.
Conflict of interest statement
The authors received no external funding for the performance of this research. All authors declare that there are no conflicts of interest concerning the materials or methods used in this study or the findings specified in this article.
Figures

References
-
- Leriche R: De I’hypotension du liquid cephalorachidien dans certaines fractures de la base du crane et de son traitment par I’injection de serum sous la peau. Lyon Chir 17: 638, 1920.
-
- Mokri B, Krueger BR, Miller GM, Piepgras DG: Meningeal gadolinium enhancement in low-pressure headaches. J Neuroimaging 3: 11– 15, 1993.
-
- Page F: Intracranial hypotension. Lancet 1: 1– 5, 1953. - PubMed
-
- Chung SJ, Kim JS, Lee MC: Syndrome of cerebral spinal fluid hypovolemia: clinical and imaging features and outcome. Neurology 55: 1321– 1327, 2000. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical