

Incretin therapies: highlighting common features and differences in the modes of action of glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors
- PMID: 26489970
- PMCID: PMC4785614
- DOI: 10.1111/dom.12591
Incretin therapies: highlighting common features and differences in the modes of action of glucagon-like peptide-1 receptor agonists and dipeptidyl peptidase-4 inhibitors
Abstract
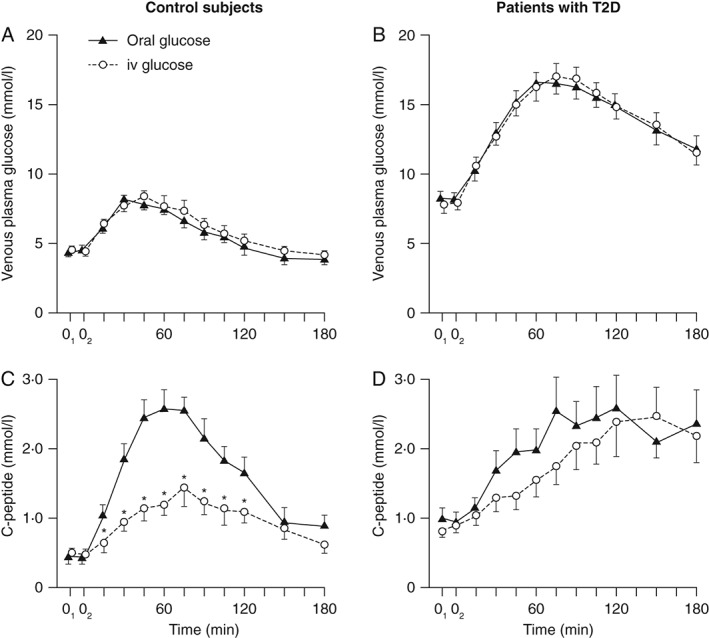
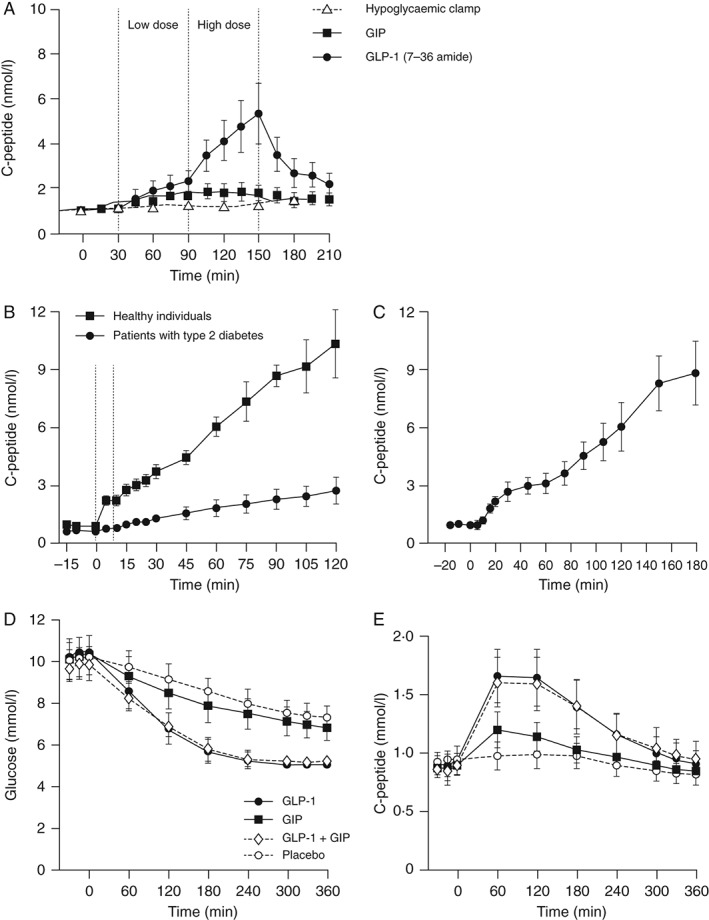
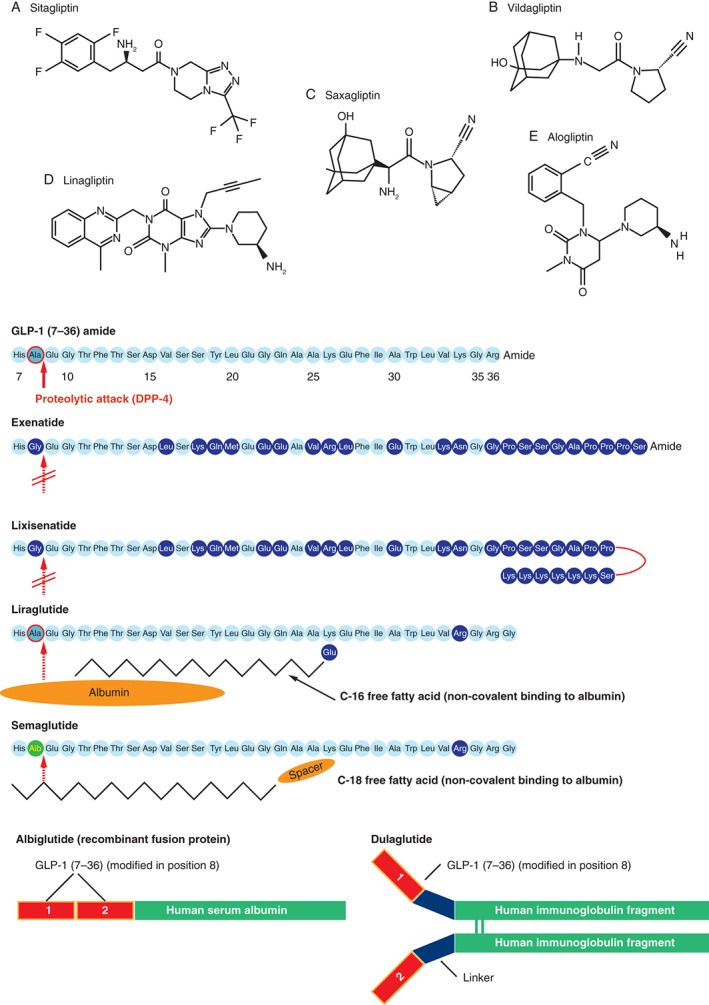
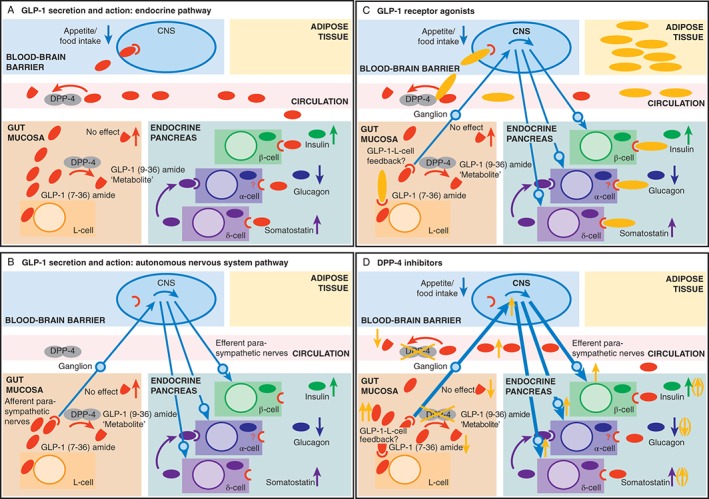
Over the last few years, incretin-based therapies have emerged as important agents in the treatment of type 2 diabetes (T2D). These agents exert their effect via the incretin system, specifically targeting the receptor for the incretin hormone glucagon-like peptide 1 (GLP-1), which is partly responsible for augmenting glucose-dependent insulin secretion in response to nutrient intake (the 'incretin effect'). In patients with T2D, pharmacological doses/concentrations of GLP-1 can compensate for the inability of diabetic β cells to respond to the main incretin hormone glucose-dependent insulinotropic polypeptide, and this is therefore a suitable parent compound for incretin-based glucose-lowering medications. Two classes of incretin-based therapies are available: GLP-1 receptor agonists (GLP-1RAs) and dipeptidyl peptidase-4 (DPP-4) inhibitors. GLP-1RAs promote GLP-1 receptor (GLP-1R) signalling by providing GLP-1R stimulation through 'incretin mimetics' circulating at pharmacological concentrations, whereas DPP-4 inhibitors prevent the degradation of endogenously released GLP-1. Both agents produce reductions in plasma glucose and, as a result of their glucose-dependent mode of action, this is associated with low rates of hypoglycaemia; however, there are distinct modes of action resulting in differing efficacy and tolerability profiles. Furthermore, as their actions are not restricted to stimulating insulin secretion, these agents have also been associated with additional non-glycaemic benefits such as weight loss, improvements in β-cell function and cardiovascular risk markers. These attributes have made incretin therapies attractive treatments for the management of T2D and have presented physicians with an opportunity to tailor treatment plans. This review endeavours to outline the commonalities and differences among incretin-based therapies and to provide guidance regarding agents most suitable for treating T2D in individual patients.
Keywords: DPP-4 inhibitor; GLP-1; GLP-1 receptor agonist; glucagon-like peptide-1; incretin enhancer; incretin mimetics; mode of action; type 2 diabetes mellitus.
© 2015 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Figures
References
-
- Ross SA. Breaking down patient and physician barriers to optimize glycemic control in type 2 diabetes. Am J Med 2013; 126: S38–S48. - PubMed
-
- Nauck MA. Unraveling the science of incretin biology. Eur J Intern Med 2009; 20(Suppl. 2): S303–S308. - PubMed
-
- Nauck M, Stockmann F, Ebert R, Creutzfeldt W. Reduced incretin effect in type 2 (non‐insulin‐dependent) diabetes. Diabetologia 1986; 29: 46–52. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
