

Diagnostic accuracy of calculated serum osmolarity to predict dehydration in older people: adding value to pathology laboratory reports
- PMID: 26490100
- PMCID: PMC4636668
- DOI: 10.1136/bmjopen-2015-008846
Diagnostic accuracy of calculated serum osmolarity to predict dehydration in older people: adding value to pathology laboratory reports
Abstract
Objectives: To assess which osmolarity equation best predicts directly measured serum/plasma osmolality and whether its use could add value to routine blood test results through screening for dehydration in older people.
Design: Diagnostic accuracy study.
Participants: Older people (≥65 years) in 5 cohorts: Dietary Strategies for Healthy Ageing in Europe (NU-AGE, living in the community), Dehydration Recognition In our Elders (DRIE, living in residential care), Fortes (admitted to acute medical care), Sjöstrand (emergency room) or Pfortmueller cohorts (hospitalised with liver cirrhosis).
Reference standard for hydration status: Directly measured serum/plasma osmolality: current dehydration (serum osmolality>300 mOsm/kg), impending/current dehydration (≥295 mOsm/kg).
Index tests: 39 osmolarity equations calculated using serum indices from the same blood draw as directly measured osmolality.
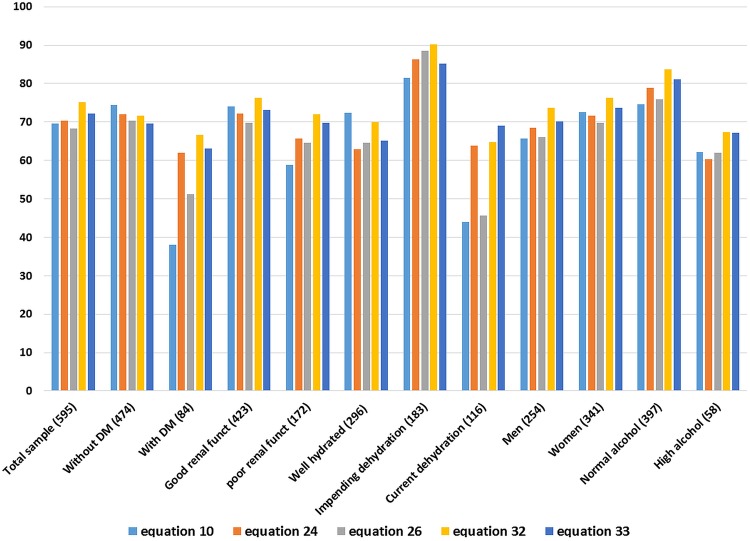
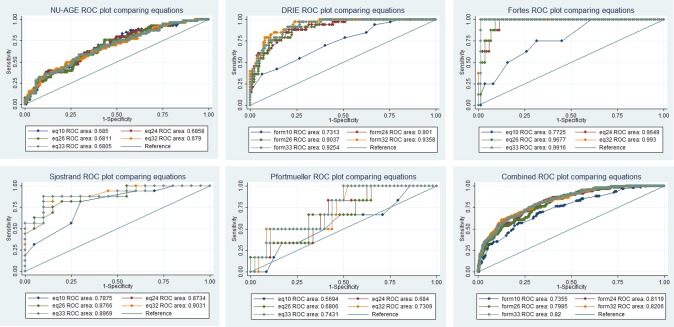
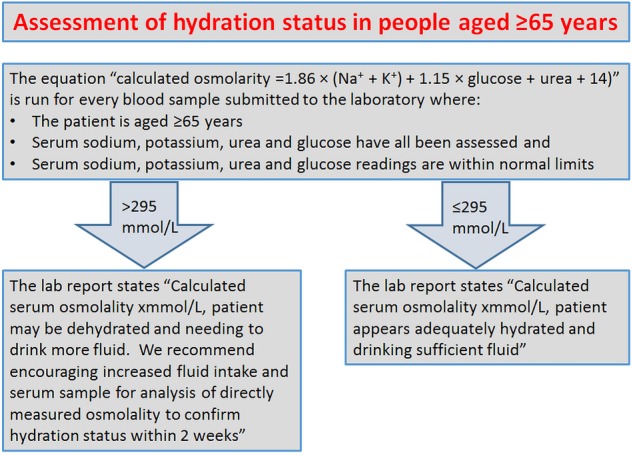
Results: Across 5 cohorts 595 older people were included, of whom 19% were dehydrated (directly measured osmolality>300 mOsm/kg). Of 39 osmolarity equations, 5 showed reasonable agreement with directly measured osmolality and 3 had good predictive accuracy in subgroups with diabetes and poor renal function. Two equations were characterised by narrower limits of agreement, low levels of differential bias and good diagnostic accuracy in receiver operating characteristic plots (areas under the curve>0.8). The best equation was osmolarity=1.86×(Na++K+)+1.15×glucose+urea+14 (all measured in mmol/L). It appeared useful in people aged ≥65 years with and without diabetes, poor renal function, dehydration, in men and women, with a range of ages, health, cognitive and functional status.
Conclusions: Some commonly used osmolarity equations work poorly, and should not be used. Given costs and prevalence of dehydration in older people we suggest use of the best formula by pathology laboratories using a cutpoint of 295 mOsm/L (sensitivity 85%, specificity 59%), to report dehydration risk opportunistically when serum glucose, urea and electrolytes are measured for other reasons in older adults.
Trial registration numbers: DRIE: Research Register for Social Care, 122273; NU-AGE: ClinicalTrials.gov NCT01754012.
Keywords: GERIATRIC MEDICINE; NUTRITION & DIETETICS; PREVENTIVE MEDICINE.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
-
- El-Sharkawy AM, Sahota O, Maughan RJ et al. Hydration in the older hospital patient—is it a problem? Age Ageing 2014;43:i33–5. 10.1093/ageing/afu046.1 - DOI
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials