

Autoimmune post-herpes simplex encephalitis of adults and teenagers
- PMID: 26491084
- PMCID: PMC4653102
- DOI: 10.1212/WNL.0000000000002125
Autoimmune post-herpes simplex encephalitis of adults and teenagers
Abstract
Objective: To report 14 patients with immune-mediated relapsing symptoms post-herpes simplex encephalitis (HSE) and to compare the clinical and immunologic features of the teenage and adult group with those of young children.
Methods: Prospective observational study of patients diagnosed between June 2013 and February 2015. Immunologic techniques have been reported previously.
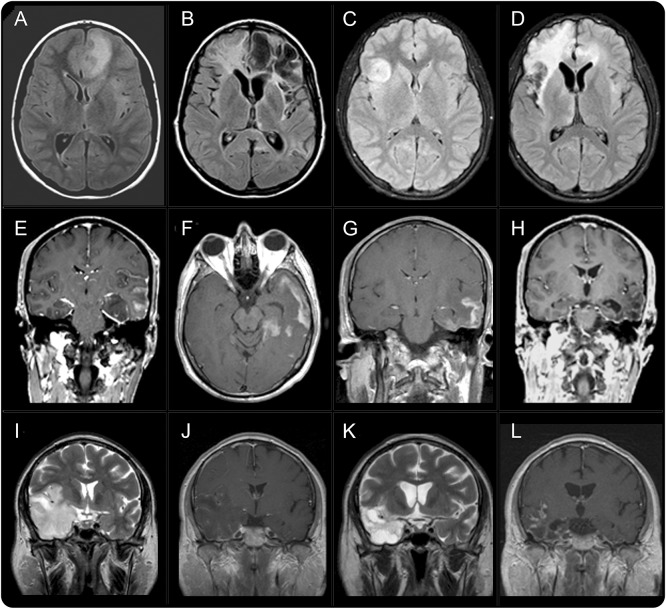
Results: Among the teenage and adult group (8 patients, median age 40 years, range 13-69; 5 male), 3 had an acute symptom presentation suggesting a viral relapse, and 5 a presentation contiguous with HSE suggesting a recrudescence of previous deficits. Seven patients developed severe psychiatric/behavioral symptoms disrupting all social interactions, and one refractory status epilepticus. Blepharospasm occurred in one patient. Five patients had CSF antibodies against NMDA receptor (NMDAR) and 3 against unknown neuronal cell surface proteins. In 5/6 patients, the brain MRI showed new areas of contrast enhancement that decreased after immunotherapy and clinical improvement. Immunotherapy was useful in 7/7 patients, sometimes with impressive recoveries, returning to their baseline HSE residual deficits. Compared with the 6 younger children (median age 13 months, range 6-20, all with NMDAR antibodies), the teenagers and adults were less likely to develop choreoathetosis (0/8 vs 6/6, p < 0.01) and decreased level of consciousness (2/8 vs 6/6, p < 0.01) and had longer delays in diagnosis and treatment (interval relapse/antibody testing 85 days, range 17-296, vs 4 days, range 0-33, p = 0.037).
Conclusion: In teenagers and adults, the immune-mediated relapsing syndrome post-HSE is different from that known in young children as choreoathetosis post-HSE and is underrecognized. Prompt diagnosis is important because immunotherapy can be highly effective.
© 2015 American Academy of Neurology.
Figures

Comment in
-
Relapse in herpes simplex virus encephalitis: It's not just about the virus.Neurology. 2015 Nov 17;85(20):1730-1. doi: 10.1212/WNL.0000000000002132. Epub 2015 Oct 21. Neurology. 2015. PMID: 26491087 No abstract available.
-
Autoimmune Post-Herpes Simplex Encephalitis.Pediatr Neurol Briefs. 2016 Mar;30(3):23. doi: 10.15844/pedneurbriefs-30-3-6. Pediatr Neurol Briefs. 2016. PMID: 27396274 Free PMC article.
References
-
- Skoldenberg B, Aurelius E, Hjalmarsson A, et al. Incidence and pathogenesis of clinical relapse after herpes simplex encephalitis in adults. J Neurol 2006;253:163–170. - PubMed
-
- Kimura H, Aso K, Kuzushima K, Hanada N, Shibata M, Morishima T. Relapse of herpes simplex encephalitis in children. Pediatrics 1992;89:891–894. - PubMed
-
- Schleede L, Bueter W, Baumgartner-Sigl S, et al. Pediatric herpes simplex virus encephalitis: a retrospective multicenter experience. J Child Neurol 2013;28:321–331. - PubMed
-
- De Tiège X, Rozenberg F, Des Portes V, et al. Herpes simplex encephalitis relapses in children: differentiation of two neurologic entities. Neurology 2003;61:241–243. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical