

Analysis of the incidence of postintubation injuries in patients intubated in the prehospital or early hospital conditions of the hospital emergency department and the intensive care unit
- PMID: 26491335
- PMCID: PMC4599039
- DOI: 10.2147/TCRM.S90181
Analysis of the incidence of postintubation injuries in patients intubated in the prehospital or early hospital conditions of the hospital emergency department and the intensive care unit
Abstract
Background: Intubation is still one of the best methods to secure the airway. In the case of prehospital or early hospital conditions when factors such as urgency, stress, or inaccuracy of the undertaken activities are involved, the risk of causing complications, for instance, edema or postintubation injuries, increases, especially while dealing with a difficult intubation. The risk of improper inflation of the endotracheal tube cuff also increases, which is considered in this study.
Objective: The aim of this study was to evaluate the prevalence of postintubation complications, such as postintubation injuries or edema, in a research sample, and to examine whether such complications occur more often, for example, while using a guidewire. In this study, we also evaluated the injuries associated with the inflation of the endotracheal tube cuff.
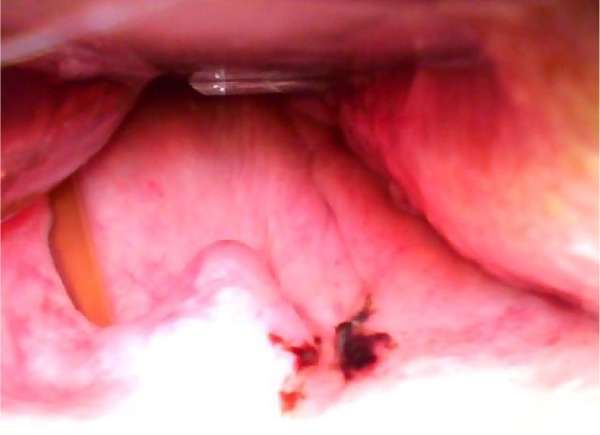
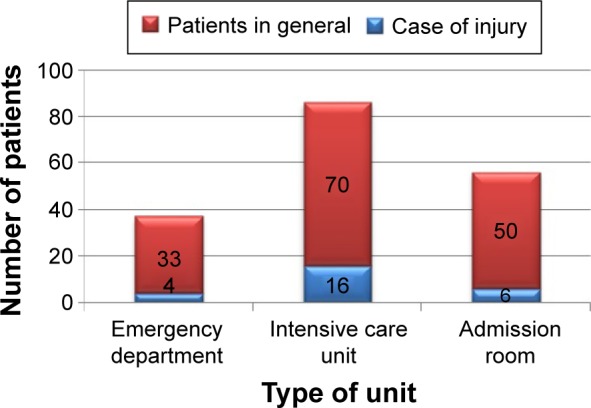
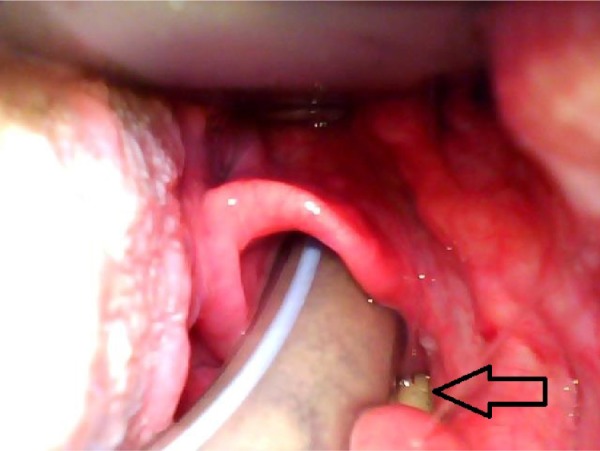
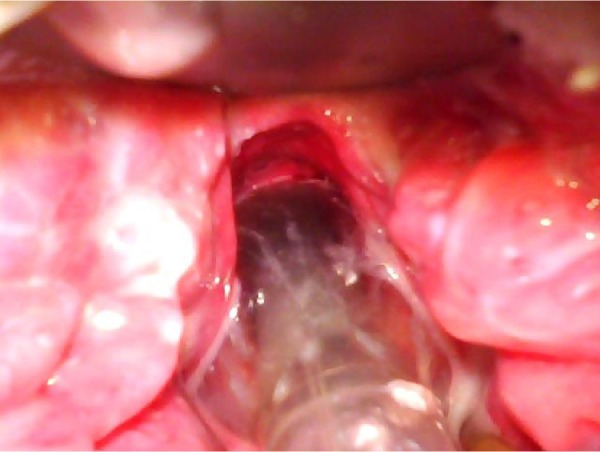
Materials and methods: This study was performed on a group of 153 patients intubated in prehospital conditions. The tests were carried out in three clinical sites that received patients from prehospital care. Postintubation injuries were revealed and photographed using videolar-yngoscope, such as the C-MAC and the McGrath series 5. The endotracheal tube cuff pressure was measured using a pressure gage manual (VBM Medizintechnik GmbH). The quantitative analyses of differences between incidence of variables were assessed using χ (2) test for P<0.05. Analyses have been carried out using the Statistica software.
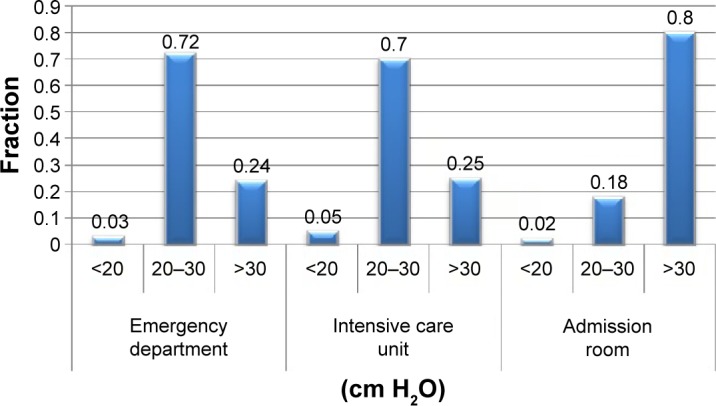
Results: In the group of 153 patients, postintubation injuries occurred in 17% of cases. The dependency between using the guidewire and the occurrence of the hematomas and loss of mucosa was statistically significant (P<0.01). In nearly half (42%) of the patients the endotracheal tube cuff pressure was excessively inflated over 30 cm H2O, and in two cases, endotracheal tube displacement was observed on account of poor cuff inflation (<20 cm H2O).
Conclusion: The highest percentage of overfilled cuffs were observed in the admission room. In the other wards, it was observed in 25% of cases. Even though only six cases of poor cuff inflation were noticed, the relationship between the leakage and the clinical conditions of patients is worth examining. The results would help in taking additional measures to reduce the risk of complications.
Keywords: endotracheal tube cuff pressure; postintubation edema; postintubation injuries.
Figures


Similar articles
-
[Analysis on risk factors of endotracheal cuff under inflation in mechanically ventilated patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014 Dec;26(12):870-4. doi: 10.3760/cma.j.issn.2095-4352.2014.12.005. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2014. PMID: 25476078 Chinese.
-
Development of appropriate procedures for inflation of endotracheal tube cuff in intubated patients.J Med Assoc Thai. 2007 Nov;90 Suppl 2:74-8. J Med Assoc Thai. 2007. PMID: 19238648
-
Evaluation of Endotracheal Tube Cuff Pressure and the Use of Three Cuff Inflation Syringe Devices in Dogs.Front Vet Sci. 2020 Feb 6;7:39. doi: 10.3389/fvets.2020.00039. eCollection 2020. Front Vet Sci. 2020. PMID: 32118062 Free PMC article.
-
Prevention of Ventilator-Associated and Early Postoperative Pneumonia Through Tapered Endotracheal Tube Cuffs: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.Crit Care Med. 2018 Feb;46(2):316-323. doi: 10.1097/CCM.0000000000002889. Crit Care Med. 2018. PMID: 29206767
-
Tracheal Injuries Complicating Prolonged Intubation and Tracheostomy.Thorac Surg Clin. 2018 May;28(2):139-144. doi: 10.1016/j.thorsurg.2018.01.001. Thorac Surg Clin. 2018. PMID: 29627046 Review.
References
-
- Raum M, Buchheisler B. The role of prehospital hypotension and respiratory dysfunction – results of epidemiological study. Abstracts of the 5th International Neurotrauma Symposium 2000. Rest Neurol Neurosci. 2000;16:265.
-
- Block E, Cheatham M, Parrish G, Nelson L. Ingested endotracheal tube in an adult following intubation attempt for head injury. Am Surg. 1999;65:1134–1136. - PubMed
-
- Nolan J. Prehospital and resuscitative airway care: should the gold standard be reassessed? Curr Opin Crit Care. 2001;7:413–421. - PubMed
-
- Murphy MF, Walls RM. The Difficult and Failed Airway. Manual of Emergency Airway Management. Philadelphia: Lippincott Williams and Wilkins; 2000. pp. 31–39.
-
- Weissbrod PA, Merati AL. Reducing injury during video-assisted endo-tracheal intubation: the “smart stylet” concept. Laryngoscope. 2011;121(11):2391–2393. - PubMed
LinkOut - more resources
Full Text Sources
