

Adult-onset Kawasaki disease (mucocutaneous lymph node syndrome) and concurrent Coxsackievirus A4 infection: a case report
- PMID: 26491373
- PMCID: PMC4599061
- DOI: 10.2147/IMCRJ.S90685
Adult-onset Kawasaki disease (mucocutaneous lymph node syndrome) and concurrent Coxsackievirus A4 infection: a case report
Abstract
Introduction: Kawasaki disease (KD) most commonly develops in infants, although its specific cause is still unclear. We report here a rare case of adult-onset KD which revealed to be concurrently infected by Coxsackievirus A4.
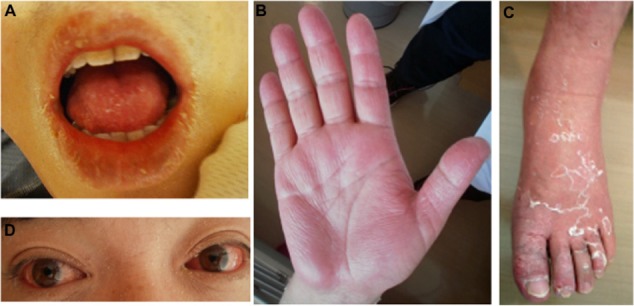
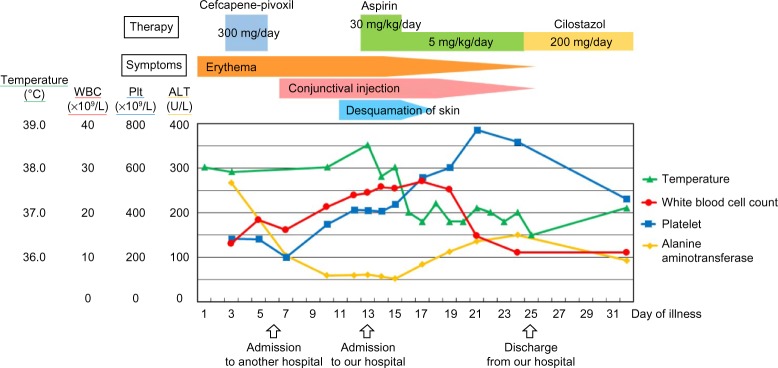
Case presentation: The patient was a 37-year-old Japanese man who presented with fever, exanthema, changes in the peripheral extremities, bilateral non-exudative conjunctival injection, and changes in the oropharynx, signs that meet the diagnostic criteria for KD defined by the Centers for Disease Control and Prevention. In this case, the patient had a significantly high antibody titer for Coxsackievirus A4, which led us to presume that the occurrence of KD was concurrent Coxsackievirus A4 infection.
Conclusion: We reported a very rare case of KD which suggests that the disease can be concurrent Coxsackievirus A4 infection. Although KD is an acute childhood disease, with fever as one of the principal features, KD should also be considered in the differential diagnosis when adult patients present with a fever of unknown cause associated with a rash.
Keywords: Coxsackievirus A4; Kawasaki disease; adult-onset; mucocutaneous lymph node syndrome; skin rash.
Figures

Similar articles
-
[Clinical details in the diagnosis of Kawasaki disease].Zhongguo Dang Dai Er Ke Za Zhi. 2022 Dec 15;24(12):1307-1310. doi: 10.7499/j.issn.1008-8830.2208124. Zhongguo Dang Dai Er Ke Za Zhi. 2022. PMID: 36544408 Free PMC article. Chinese.
-
Kawasaki disease in children and adolescents: clinical data of Kawasaki patients in a western region (Tyrol) of Austria from 2003-2012.Pediatr Rheumatol Online J. 2014 Sep 2;12(1):37. doi: 10.1186/1546-0096-12-37. Pediatr Rheumatol Online J. 2014. PMID: 27643389 Free PMC article.
-
Kawasaki disease: A brief history.Pediatrics. 2000 Aug;106(2):E27. doi: 10.1542/peds.106.2.e27. Pediatrics. 2000. PMID: 10920183 Review.
-
Twenty-year-old woman presenting with typical Kawasaki disease.Dermatol Online J. 2019 Jul 15;25(7):13030/qt38c0f8gf. Dermatol Online J. 2019. PMID: 31450283
-
Kawasaki Disease in the neonate: case report and literature review.Pediatr Rheumatol Online J. 2018 Jul 3;16(1):43. doi: 10.1186/s12969-018-0263-8. Pediatr Rheumatol Online J. 2018. PMID: 29970110 Free PMC article. Review.
Cited by
-
Multisystem Inflammatory Syndrome in Children in New York State.N Engl J Med. 2020 Jul 23;383(4):347-358. doi: 10.1056/NEJMoa2021756. Epub 2020 Jun 29. N Engl J Med. 2020. PMID: 32598830 Free PMC article.
-
Pustules on the back possibly triggering toxic-shock syndrome.BMJ Case Rep. 2019 Jun 29;12(6):e229610. doi: 10.1136/bcr-2019-229610. BMJ Case Rep. 2019. PMID: 31256050 Free PMC article.
-
Genome Analysis of Coxsackievirus A4 Isolates From Hand, Foot, and Mouth Disease Cases in Shandong, China.Front Microbiol. 2019 May 7;10:1001. doi: 10.3389/fmicb.2019.01001. eCollection 2019. Front Microbiol. 2019. PMID: 31134033 Free PMC article.
-
Simultaneous development of Kawasaki disease following acute human adenovirus infection in monozygotic twins: A case report.Pediatr Rheumatol Online J. 2017 May 16;15(1):39. doi: 10.1186/s12969-017-0169-x. Pediatr Rheumatol Online J. 2017. PMID: 28511718 Free PMC article.
-
Atypical Kawasaki Disease after COVID-19 Vaccination: A New Form of Adverse Event Following Immunization.Vaccines (Basel). 2022 Jan 16;10(1):126. doi: 10.3390/vaccines10010126. Vaccines (Basel). 2022. PMID: 35062787 Free PMC article.
References
-
- Kawasaki T. Acute febrile muco-cutaneous lymph node syndrome in young children with unique digital desquamation. Jpn J Allergol. 1967;16:178–222.
-
- Yanagawa H, Kawasaki T, Shigematsu I. Nationwide survey on Kawasaki disease in Japan. Pediatrics. 1987;80:58–62. - PubMed
-
- Rauch AM. Kawasaki syndrome: critical review of US epidemiology. Prog Clin Biol Res. 1987;250:33–40. - PubMed
-
- Jackson JL, Kunkel MR, Libow L, Gates RH. Adult Kawasaki disease. Report of two cases treated with intravenous gamma globulin. Arch Intern Med. 1994;154:1398–1405. - PubMed
-
- Hall M, Hoyt L, Ferrieri P, Schlievert PM, Jenson HB. Kawasaki syndrome-like illness associated with infection caused by enterotoxin B-secreting Staphylococcus aureus. Clin Infect Dis. 1999;29:586–589. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
