

Nonalcoholic Steatohepatitis Is Associated With Increased Mortality in Obese Patients Undergoing Bariatric Surgery
- PMID: 26492845
- PMCID: PMC4838546
- DOI: 10.1016/j.cgh.2015.10.010
Nonalcoholic Steatohepatitis Is Associated With Increased Mortality in Obese Patients Undergoing Bariatric Surgery
Abstract
Background & aims: Bariatric surgery is associated with improved outcomes in subjects with severe obesity. We investigated the prognostic relevance of nonalcoholic steatohepatitis (NASH) and liver gene expression patterns in patients undergoing bariatric surgery.
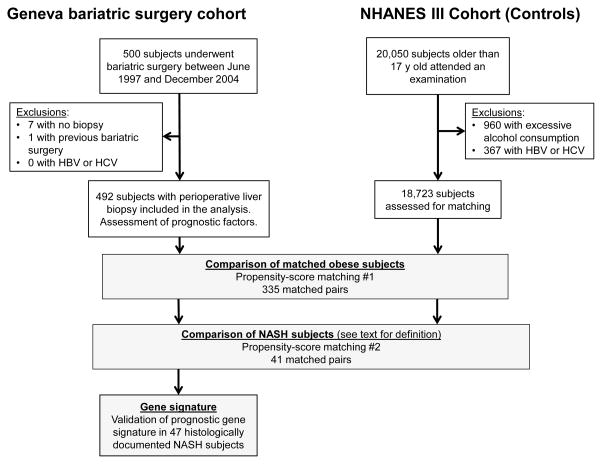
Methods: We performed a retrospective analysis of 492 subjects who underwent gastric bypass bariatric surgery at a single center in Switzerland from January 1997 through December 2004; routine perioperative liver biopsies were collected, analyzed histologically, and RNA was isolated. We collected data on overall survival and clinical and biochemical parameters and compared these with data from propensity score-matched subjects participating in the third National Health and Nutrition Examination Survey (NHANES III). We used liver biopsies to identify bariatric surgery patients with NASH; NHANES III participants with NASH were identified based on a hyperechogenic liver at ultrasound and increased alanine transaminase levels. We analyzed a 32-gene signature associated with NAFLD severity in the liver tissues collected from 47 bariatric surgery patients with NASH, and assessed its prognostic features using nearest template prediction and survival analysis.
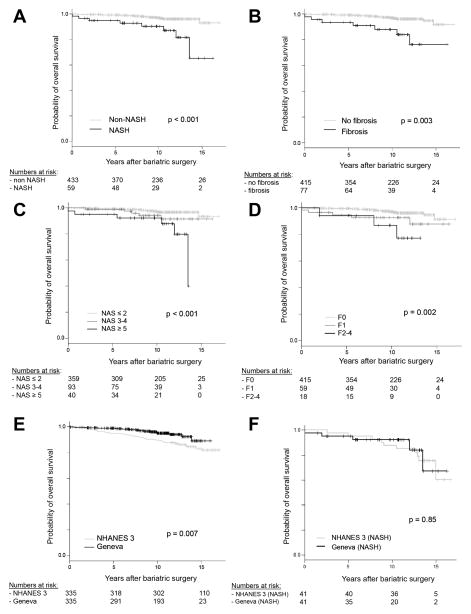
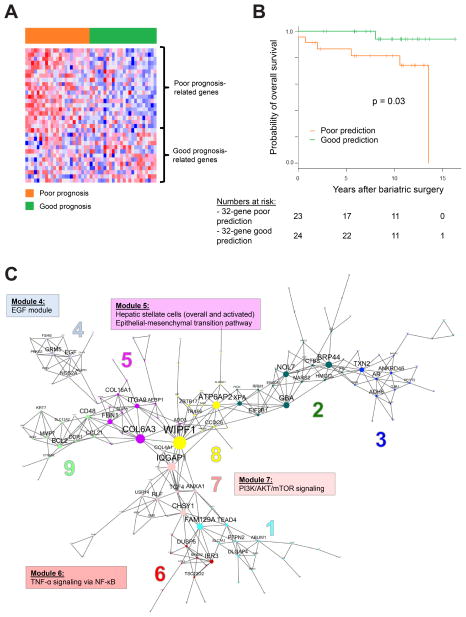
Results: At baseline, the median body mass index of patients who underwent bariatric surgery was 43.6 kg/m2; based on histologic findings, 12% had NASH and 16% had fibrosis. During a median follow-up of 10.2 years after the surgery, 4.2% of the subjects died. In multivariable Cox regression, the presence of NASH (hazard ratio [HR], 2.9; P = .02) and arterial hypertension (HR, 3.9; P = .02) were associated with overall mortality. When bariatric surgery patients were matched with NHANES III participants, bariatric surgery reduced the risk of death during the follow-up period (HR, 0.54; P = .04). However, bariatric surgery patients with NASH did not have a reduced risk of death compared with NHANES III participants with NASH (HR, 0.90; P = .85). We identified an expression pattern of 32 genes in liver tissues from patients with NASH that was associated with increased risk of death in multivariable analysis (HR, 7.7; P = .045).
Conclusions: Histologically proven NASH is associated with increased risk of death within a median follow-up of 10.2 years after bariatric surgery, compared with patients who undergo bariatric surgery without NASH. The survival benefit of bariatric surgery in subjects with NASH may be reduced. A 32-gene expression pattern identified patients with NASH who underwent bariatric surgery and had shorter survival times.
Keywords: Biomarker; Fatty Liver Disease; NHANES III; Postoperative Complication; Treatment.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors disclose no conflicts
Figures
References
-
- Finkelstein EA, Trogdon JG, Cohen JW, et al. Annual Medical Spending Attributable To Obesity: Payer-And Service-Specific Estimates. Health Affairs. 2009;28(5):w822–w31. - PubMed
-
- Browning JD, Szczepaniak LS, Dobbins R, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387–95. - PubMed
-
- Loomba R, Sanyal AJ. The global NAFLD epidemic. Nat Rev Gastroenterol Hepatol. 2013;10(11):686–90. Epub 2013/09/18. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
