

District-level hospital trauma care audit filters: Delphi technique for defining context-appropriate indicators for quality improvement initiative evaluation in developing countries
- PMID: 26492882
- PMCID: PMC4698059
- DOI: 10.1016/j.injury.2015.09.007
District-level hospital trauma care audit filters: Delphi technique for defining context-appropriate indicators for quality improvement initiative evaluation in developing countries
Abstract
Introduction: Prospective clinical audit of trauma care improves outcomes for the injured in high-income countries (HICs). However, equivalent, context-appropriate audit filters for use in low- and middle-income country (LMIC) district-level hospitals have not been well established. We aimed to develop context-appropriate trauma care audit filters for district-level hospitals in Ghana, was well as other LMICs more broadly.
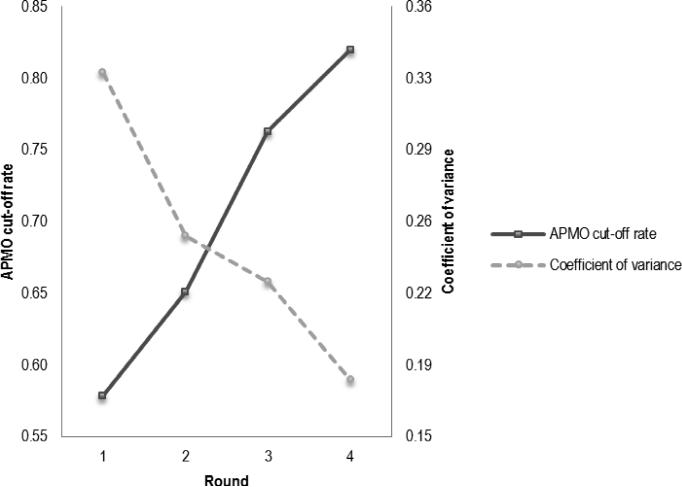
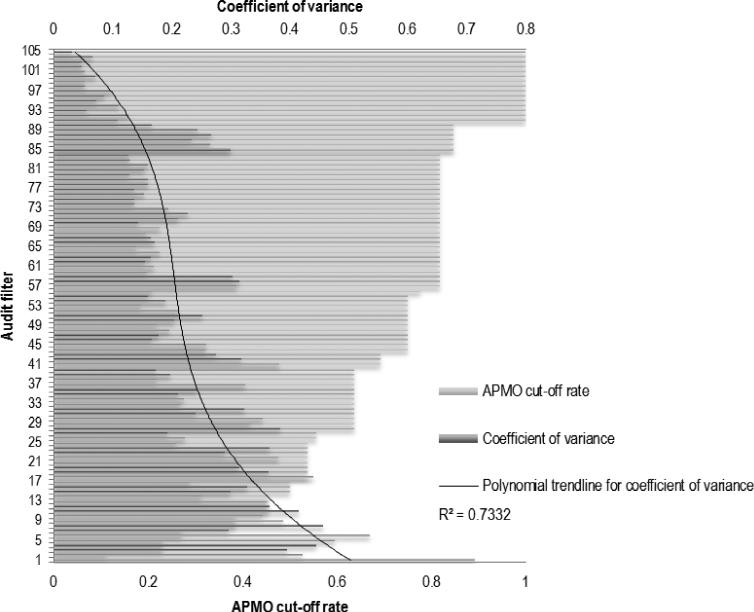
Methods: Consensus on trauma care audit filters was built between twenty panellists using a Delphi technique with four anonymous, iterative surveys designed to elicit: (i) trauma care processes to be measured; (ii) important features of audit filters for the district-level hospital setting; and (iii) potentially useful filters. Filters were ranked on a scale from 0 to 10 (10 being very useful). Consensus was measured with average percent majority opinion (APMO) cut-off rate. Target consensus was defined a priori as: a median rank of ≥9 for each filter and an APMO cut-off rate of ≥0.8.
Results: Panellists agreed on trauma care processes to target (e.g. triage, phases of trauma assessment, early referral if needed) and specific features of filters for district-level hospital use (e.g. simplicity, unassuming of resource capacity). APMO cut-off rate increased successively: Round 1--0.58; Round 2--0.66; Round 3--0.76; and Round 4--0.82. After Round 4, target consensus on 22 trauma care and referral-specific filters was reached. Example filters include: triage--vital signs are recorded within 15 min of arrival (must include breathing assessment, heart rate, blood pressure, oxygen saturation if available); circulation--a large bore IV was placed within 15 min of patient arrival; referral--if referral is activated, the referring clinician and receiving facility communicate by phone or radio prior to transfer.
Conclusion: This study proposes trauma care audit filters appropriate for LMIC district-level hospitals. Given the successes of similar filters in HICs and obstetric care filters in LMICs, the collection and reporting of prospective trauma care audit filters may be an important step towards improving care for the injured at district-level hospitals in LMICs.
Keywords: Developing country; Ghana; Global surgery; Quality improvement; Trauma.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Perceived usefulness of trauma audit filters in urban India: a mixed-methods multicentre Delphi study comparing filters from the WHO and low and middle-income countries.BMJ Open. 2022 Jun 9;12(6):e059948. doi: 10.1136/bmjopen-2021-059948. BMJ Open. 2022. PMID: 35680271 Free PMC article.
-
Developing Trauma Audit Filters for Regional Referral Hospitals in Cameroon: Mixed-Methods Approach.J Surg Res. 2018 Dec;232:578-586. doi: 10.1016/j.jss.2018.07.048. Epub 2018 Aug 8. J Surg Res. 2018. PMID: 30463777
-
The identification of criteria to evaluate prehospital trauma care using the Delphi technique.J Trauma. 2007 Mar;62(3):708-13. doi: 10.1097/01.ta.0000197150.07714.c2. J Trauma. 2007. PMID: 17414352
-
Surgical and trauma care in low- and middle-income countries: a review of capacity assessments.J Surg Res. 2017 Apr;210:139-151. doi: 10.1016/j.jss.2016.11.005. Epub 2016 Nov 10. J Surg Res. 2017. PMID: 28457320
-
Trauma audit and quality improvement.Aust N Z J Surg. 1994 Mar;64(3):147-54. doi: 10.1111/j.1445-2197.1994.tb02168.x. Aust N Z J Surg. 1994. PMID: 8117190 Review.
Cited by
-
Perceived usefulness of trauma audit filters in urban India: a mixed-methods multicentre Delphi study comparing filters from the WHO and low and middle-income countries.BMJ Open. 2022 Jun 9;12(6):e059948. doi: 10.1136/bmjopen-2021-059948. BMJ Open. 2022. PMID: 35680271 Free PMC article.
-
Building Trauma and EMS Systems Capacity in Rwanda: Lessons and Recommendations.Ann Glob Health. 2021 Oct 26;87(1):104. doi: 10.5334/aogh.3324. eCollection 2021. Ann Glob Health. 2021. PMID: 34754760 Free PMC article.
-
Consensus recommendations for essential vascular care in low- and middle-income countries.J Vasc Surg. 2016 Dec;64(6):1770-1779.e1. doi: 10.1016/j.jvs.2016.05.046. Epub 2016 Jul 16. J Vasc Surg. 2016. PMID: 27432199 Free PMC article.
-
Differences in trauma care between district and regional hospitals and impact of a trauma intake form with decision support prompts in Ghana: A stepped-wedge cluster randomized trial.World J Surg. 2024 Mar;48(3):527-539. doi: 10.1002/wjs.12082. Epub 2024 Feb 5. World J Surg. 2024. PMID: 38312029 Free PMC article. Clinical Trial.
-
Injured and broke: The impacts of the Ghana National Health Insurance Scheme (NHIS) on service delivery and catastrophic health expenditure among seriously injured children.Afr J Emerg Med. 2021 Mar;11(1):144-151. doi: 10.1016/j.afjem.2020.09.013. Epub 2020 Nov 16. Afr J Emerg Med. 2021. PMID: 33680736 Free PMC article.
References
-
- Data VisualizationsGlobal Burden of Disease Cause Patterns. Institute of Health Metrics and Evaluation; Seattle, WA: 2013.
-
- Wong EG, Gupta S, Deckelbaum DL, Razek T, Kushner AL. Prioritizing injury care: a review of trauma capacity in low and middle-income countries. Journal of Surgical Research. 2014 - PubMed
-
- Stelfox HT, Joshipura M, Chadbunchachai W, Ellawala RN, O'Reilly G, Nguyen TS, et al. Trauma quality improvement in low and middle income countries of the Asia-Pacific region: a mixed methods study. World journal of surgery. 2012;36:1978–1992. - PubMed
-
- Mock C, Julliard C, Brundage S, Goosen J, Joshipura M. Guidelines for trauma quality improvement programmes. World Health Organization; Geneva: 2009.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
