

The Royal College of Ophthalmologists' National Ophthalmology Database Study of cataract surgery: report 2, relationships of axial length with ocular copathology, preoperative visual acuity, and posterior capsule rupture
- PMID: 26493034
- PMCID: PMC5129808
- DOI: 10.1038/eye.2015.198
The Royal College of Ophthalmologists' National Ophthalmology Database Study of cataract surgery: report 2, relationships of axial length with ocular copathology, preoperative visual acuity, and posterior capsule rupture
Abstract
Purpose: To describe the relationships of axial length with ocular copathology, preoperative visual acuity, and posterior capsule rupture rates in patients undergoing cataract surgery.DesignThe Royal College of Ophthalmologists' National Ophthalmology Database (NOD) study.
Methods: Anonymised data on 180 114 eyes from 127 685 patients undergoing cataract surgery between August 2006 and November 2010 were collected prospectively from 28 sites. Data parameters included: demographics, biometry, ocular copathology, visual acuity measurements, and surgical complications including posterior capsule rupture, or vitreous loss or both (PCR).
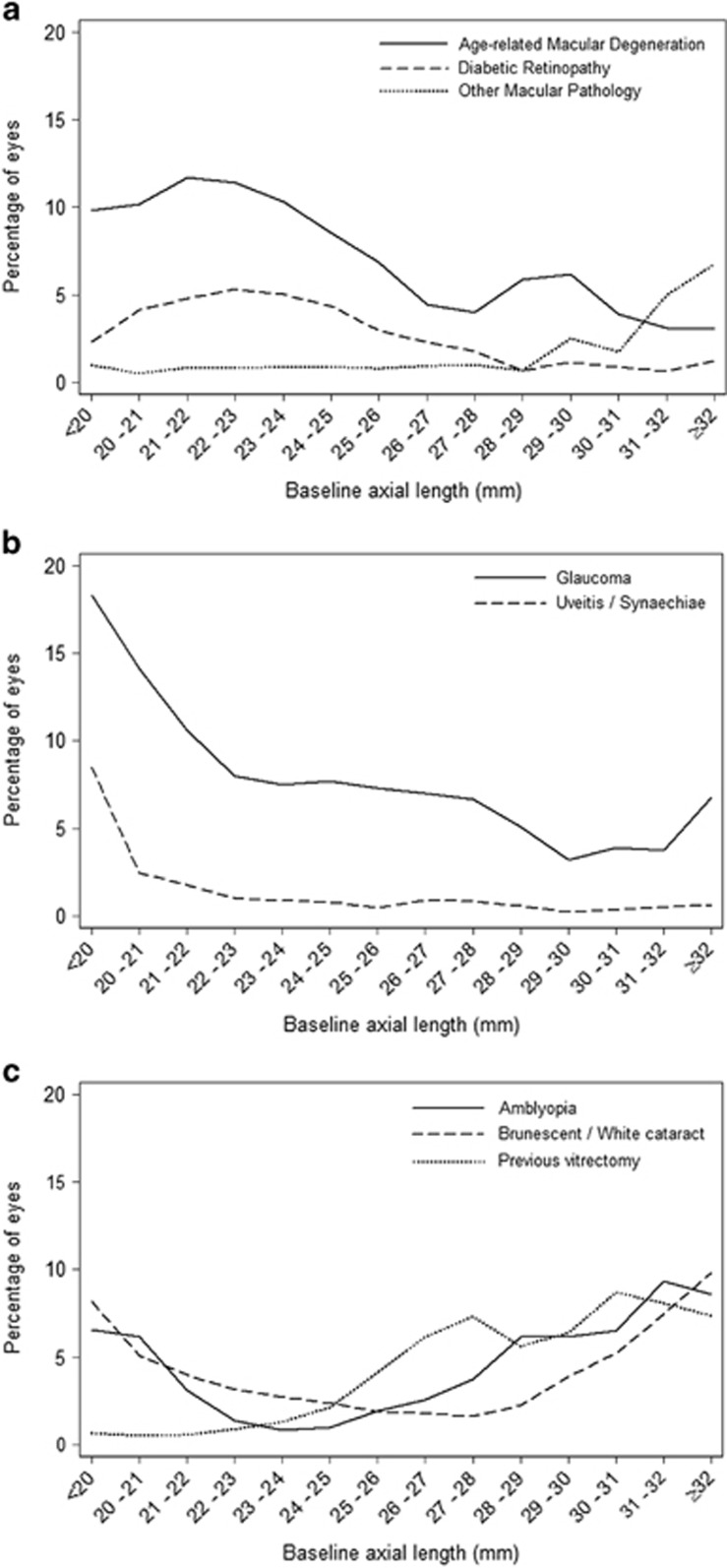
Results: Consultant surgeons performed a higher proportion of operations on eyes whose axial length were at the extremes. Glaucoma and age related macular degeneration were more common in eyes with shorter axial lengths, whilst previous vitrectomy was associated with longer axial lengths. Eyes with brunescent or white cataracts or amblyopia were more common at both axial length extremes. Preoperative visual acuities were similar for eyes with axial length measurements up to approximately 28 mm and worse for eyes with longer axial length measurements. PCR rates showed little change with axial length (overall mean 1.95%, 95% CI: 1.89 to 2.01%), except for a borderline increase in eyes with axial length <20.0 mm where rates were 3.6% (95% CI: 2.0 to 6.3%). The likelihood of PCR in eyes with axial length <20.0 mm was 1.88 times higher than those of ≥20.0 mm (P=0.0373).
Conclusion: Rates of ocular comorbidities vary by axial length. PCR rates in eyes with very short or long axial lengths were lower than expected.
Conflict of interest statement
PHJD's employer received unrestricted funding from The Special Trustees of Moorfield's Eye Hospital to analyse these data. RLJ is the Medical Director of Medisoft Limited, which developed the electronic medical record from which data were extracted, for the first iteration of the National Ophthalmology Database. The remaining authors declare no conflict of interest.
Figures

Similar articles
-
The Royal College of Ophthalmologists' National Ophthalmology Database Study of cataract surgery. Report 5: Clinical outcome and risk factors for posterior capsule rupture and visual acuity loss following cataract surgery in patients aged 90 years and older.Eye (Lond). 2019 Jul;33(7):1161-1170. doi: 10.1038/s41433-019-0389-z. Epub 2019 Mar 11. Eye (Lond). 2019. PMID: 30858564 Free PMC article.
-
The Royal College of Ophthalmologists' National Ophthalmology Database study of cataract surgery: Report 17, a risk factor model for posterior capsule rupture.Eye (Lond). 2024 Dec;38(18):3495-3503. doi: 10.1038/s41433-024-03344-2. Epub 2024 Sep 19. Eye (Lond). 2024. PMID: 39294232
-
The Royal College of Ophthalmologists' National Ophthalmology Database study of cataract surgery: report 1, visual outcomes and complications.Eye (Lond). 2015 Apr;29(4):552-60. doi: 10.1038/eye.2015.3. Epub 2015 Feb 13. Eye (Lond). 2015. PMID: 25679413 Free PMC article.
-
Intraoperative management of posterior capsular rupture.Curr Opin Ophthalmol. 2015 Jan;26(1):16-21. doi: 10.1097/ICU.0000000000000113. Curr Opin Ophthalmol. 2015. PMID: 25390858 Review.
-
Visual outcome following posterior capsule rupture during manual small incision cataract surgery.Niger J Clin Pract. 2021 Jun;24(6):948-953. doi: 10.4103/njcp.njcp_272_20. Niger J Clin Pract. 2021. PMID: 34121746 Review.
Cited by
-
Surgical planning during a pandemic: Identifying patients at high risk of severe disease or death due to COVID-19 in a cohort of patients on a cataract surgery waiting list.Ulster Med J. 2022 Jan;91(1):19-25. Epub 2022 Feb 11. Ulster Med J. 2022. PMID: 35169334 Free PMC article.
-
Practical Algorithm Evaluating Preoperative Risk Factors for Posterior Capsule Rupture During Phacoemulsification.Cureus. 2025 Feb 12;17(2):e78907. doi: 10.7759/cureus.78907. eCollection 2025 Feb. Cureus. 2025. PMID: 40091986 Free PMC article.
-
In-depth analysis of risk factors for pseudophakic retinal detachments and retinal breaks.Acta Ophthalmol. 2022 May;100(3):e694-e700. doi: 10.1111/aos.14974. Epub 2021 Jul 13. Acta Ophthalmol. 2022. PMID: 34258879 Free PMC article.
-
Royal College of Ophthalmologists' National Ophthalmology Database study of cataract surgery: report 8, cohort analysis of the relationship between intraoperative complications of cataract surgery and axial length.BMJ Open. 2022 Aug 19;12(8):e053560. doi: 10.1136/bmjopen-2021-053560. BMJ Open. 2022. PMID: 35985773 Free PMC article.
-
Reviewing the visual benefits of femtosecond laser-assisted cataract surgery: Can we improve our outcomes?Indian J Ophthalmol. 2017 Dec;65(12):1314-1322. doi: 10.4103/ijo.IJO_736_17. Indian J Ophthalmol. 2017. PMID: 29208811 Free PMC article. Review.
References
-
- Jaycock P, Johnston RL, Taylor H, Adams M, Tole DM, Galloway P et al. The Cataract National Dataset electronic multi-centre audit of 55 567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye 2009; 23(1): 38–49. - PubMed
-
- Johnston RL, Taylor H, Smith R, Sparrow JM. The Cataract National Dataset Electronic Multi-centre Audit of 55 567 Operations: variation in posterior capsule rupture rates between surgeons. Eye (Lond) 2010; 24(5): 888–893. - PubMed
-
- Knox Cartwright NE, Johnston RL, Jaycock PD, Tole DM, Sparrow JM. The Cataract National Dataset electronic multicentre audit of 55 567 operations: when should IOLMaster biometric measurements be rechecked? Eye (Lond) 2010; 24(5): 894–900. - PubMed
-
- Narendran N, Jaycock P, Johnston RL, Taylor H, Adams M, Tole DM et al. The Cataract National Dataset electronic multicentre audit of 55 567 operations: risk stratification for posterior capsule rupture and vitreous loss. Eye 2009; 23(1): 31–37. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
