

Primary posterior continuous curvilinear capsulorhexis combined with diffractive multifocal intraocular lens implantation
- PMID: 26493036
- PMCID: PMC4709543
- DOI: 10.1038/eye.2015.201
Primary posterior continuous curvilinear capsulorhexis combined with diffractive multifocal intraocular lens implantation
Abstract
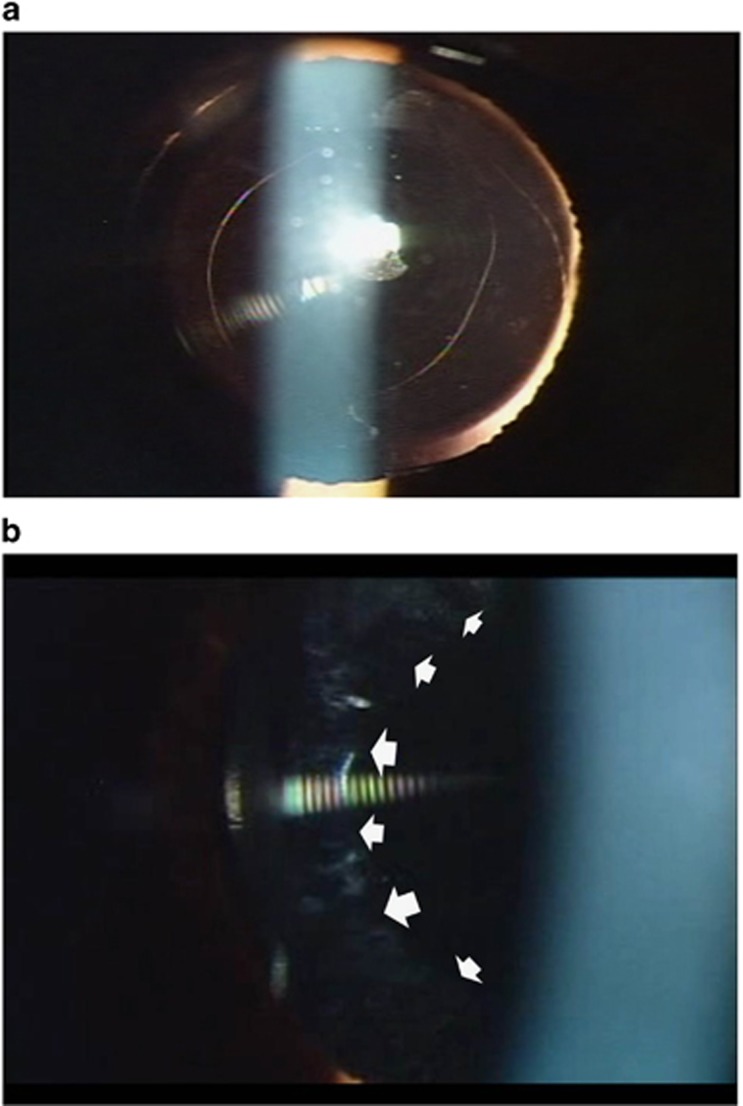
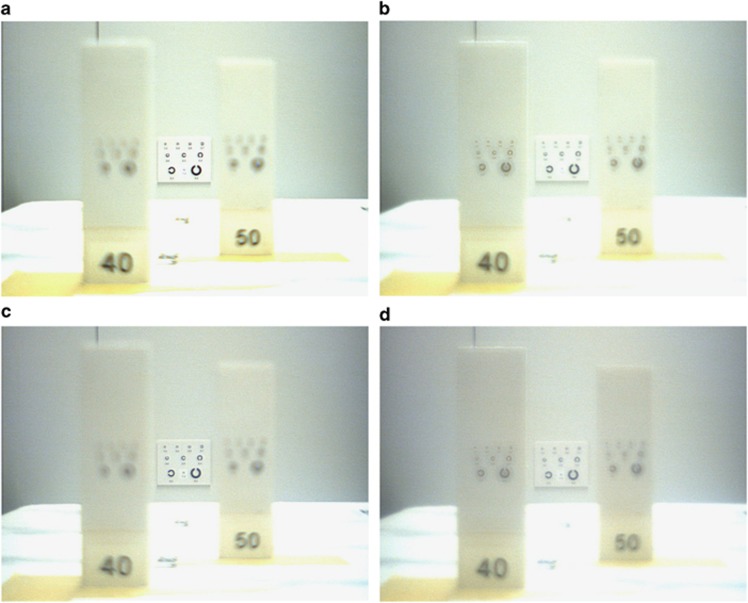
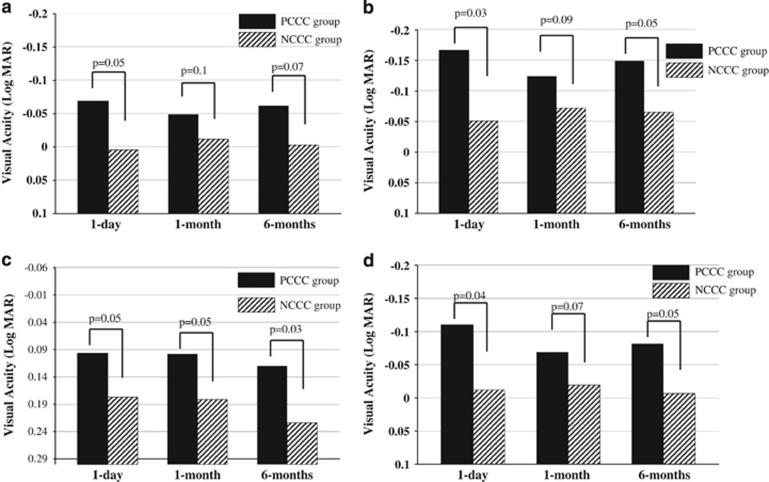
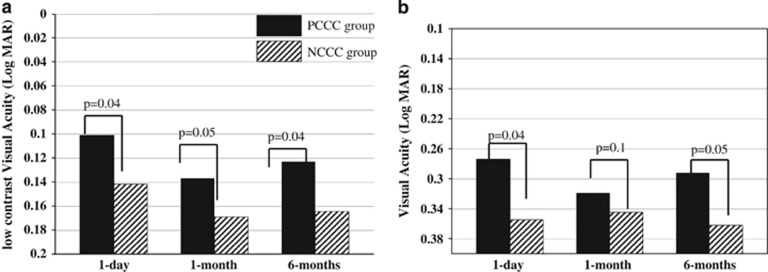
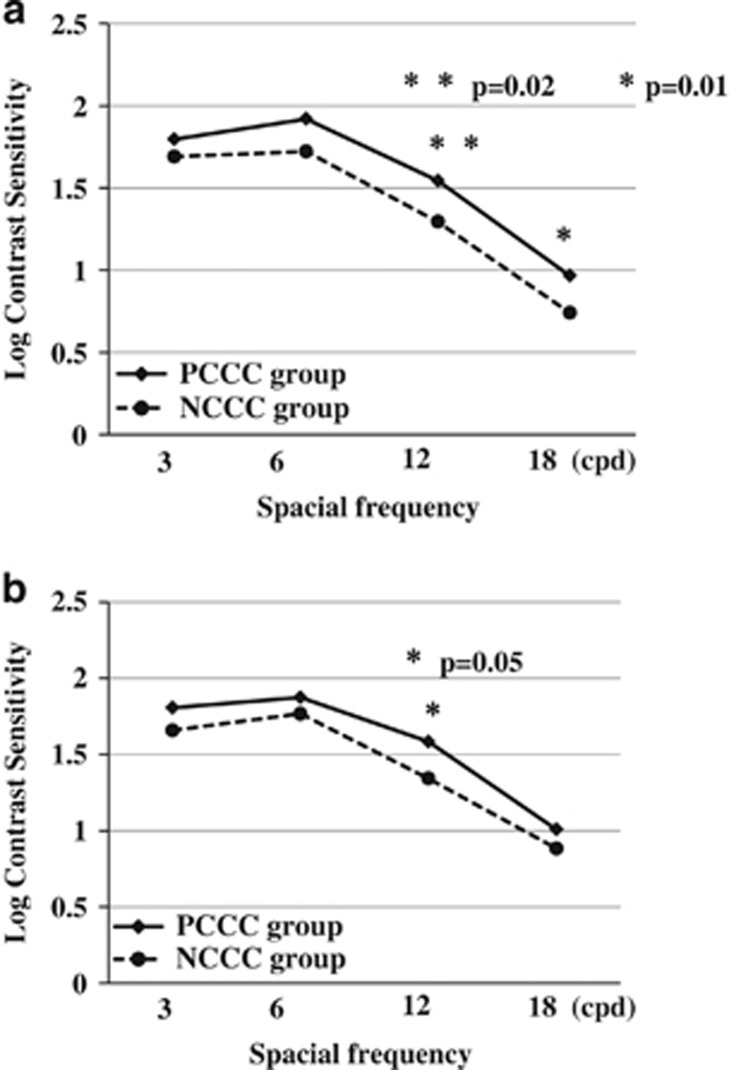
PurposeTo evaluate the effect of mild posterior capsule opacity (PCO) on visual acuity (VA) in eyes implanted with a diffractive multifocal intraocular lens (IOL) compared with a monofocal IOL, and the effect of posterior continuous curvilinear capsulorhexis (PCCC) combined with diffractive multifocal IOL implantation.MethodsFor the initial evaluation, we compared charge-coupled device (CCD) camera photographs taken through both a monofocal IOL-loaded model eye and a diffractive IOL-loaded model eye under the conditions of both with and without an opaque filter for the simulation of mild PCO. The clinical evaluation involved 20 patients who underwent bilateral implantation of the same diffractive multifocal IOL. In all 20 cases, PCCC was performed in 1 eye (PCCC group) and not performed in the fellow eye (NCCC group). Postoperative clinical results were then compared between the two groups.ResultsThe CCD photographs revealed that the diffractive IOL-loaded eye was more strongly affected by the simulated PCO than was the monofocal IOL-loaded eye. In the clinical setting, the PCCC group registered better results than NCCC group in distance and near VA, low-contrast VA, and contrast sensitivity testing.ConclusionsDiffractive multifocal IOLs tend to be more influenced by mild PCO than do monofocal IOLs, and PCCC prior to IOL implantation can contribute to the avoidance of this effect.
Figures
References
-
- 1Souza CE, Gerente VM, Chalita MR, Soriano ES, Freitas LL, Belfort R Jr.. Visual acuity, contrast sensitivity, reading speed, and wavefront analysis: pseudophakic eye with multifocal IOL (ReSTOR) versus fellow phakic eye in non-presbyopic patients. J Refract Surg 2006; 22: 303–305. - PubMed
-
- 2Vingolo EM, Grenga P, Iacobelli L, Grenga R. Visual acuity and contrast sensitivity: AcrySof ReSTOR apodized diffractive versus AcrySof SA60AT monofocal intraocular lenses. J Cataract Refract Surg 2007; 33: 1244–1247. - PubMed
-
- 3Blaylock JF, Si Z, Aitchison S, Prescott C. Visual function and change in quality of life after bilateral refractive lens exchange with the ReSTOR multifocal intraocular lens. J Refract Surg 2008; 24: 265–273. - PubMed
-
- 5de Vries NE, Webers CA, Touwslager WR, Bauer NJ, de Brabander J, Berendschot TT, Nuijts RM. Dissatisfaction after implantation of multifocal intraocular lenses. J Cataract Refract Surg 2011; 37: 859–865. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
