

Comparison of Prostate-Specific Membrane Antigen-Based 18F-DCFBC PET/CT to Conventional Imaging Modalities for Detection of Hormone-Naïve and Castration-Resistant Metastatic Prostate Cancer
- PMID: 26493203
- PMCID: PMC4730886
- DOI: 10.2967/jnumed.115.163782
Comparison of Prostate-Specific Membrane Antigen-Based 18F-DCFBC PET/CT to Conventional Imaging Modalities for Detection of Hormone-Naïve and Castration-Resistant Metastatic Prostate Cancer
Abstract
Conventional imaging modalities (CIMs) have limited sensitivity and specificity for detection of metastatic prostate cancer. We examined the potential of a first-in-class radiofluorinated small-molecule inhibitor of prostate-specific membrane antigen (PSMA), N-[N-[(S)-1,3-dicarboxypropyl]carbamoyl]-4-(18)F-fluorobenzyl-l-cysteine ((18)F-DCFBC), to detect metastatic hormone-naïve (HNPC) and castration-resistant prostate cancer (CRPC).
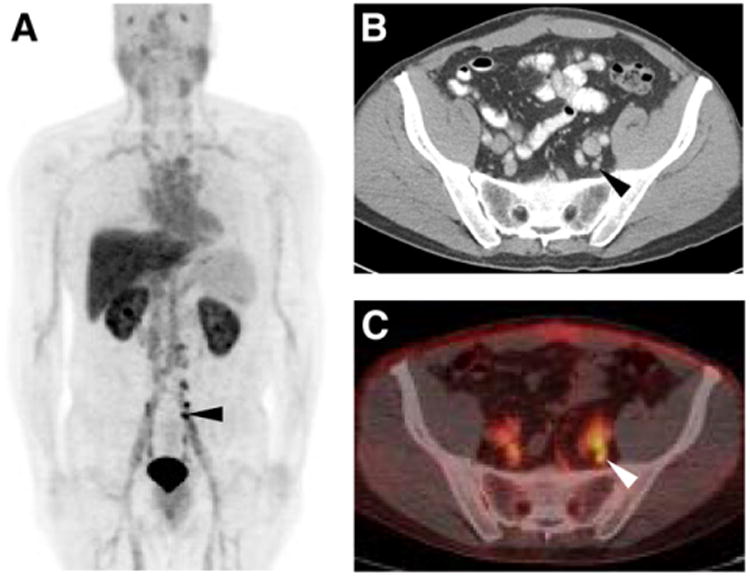
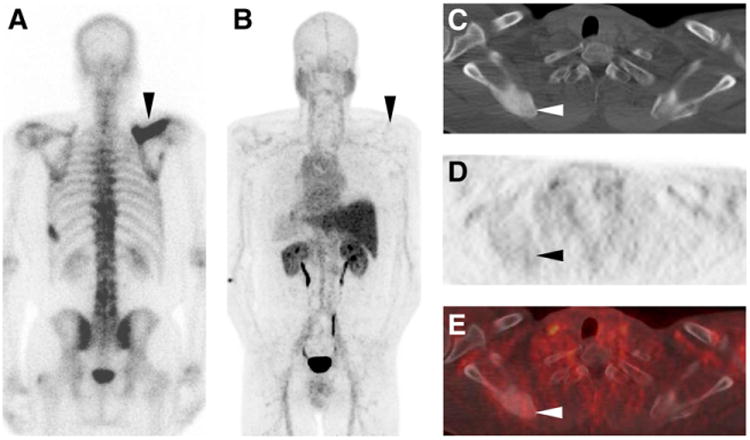
Methods: Seventeen patients were prospectively enrolled (9 HNPC and 8 CRPC); 16 had CIM evidence of new or progressive metastatic prostate cancer and 1 had high clinical suspicion of metastatic disease. (18)F-DCFBC PET/CT imaging was obtained with 2 successive PET scans starting at 2 h after injection. Patients were imaged with CIM at approximately the time of PET. A lesion-by-lesion analysis of PET to CIM was performed in the context of either HNPC or CRPC. The patients were followed with available clinical imaging as a reference standard to determine the true nature of identified lesions on PET and CIM.
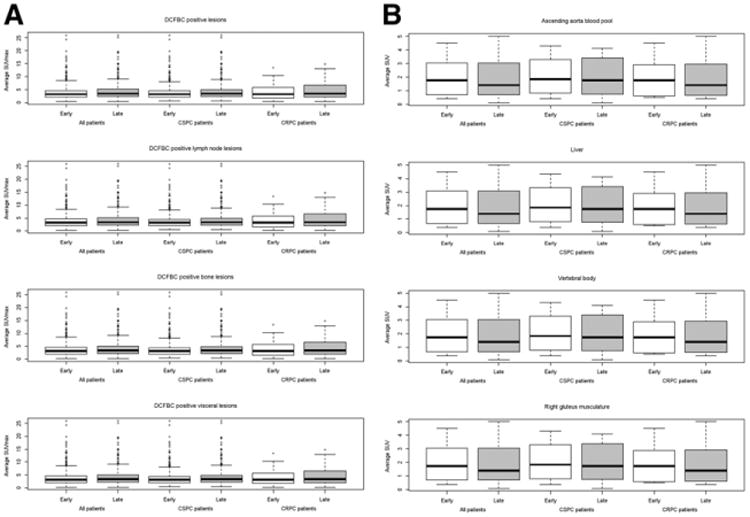
Results: On the lesion-by-lesion analysis, (18)F-DCFBC PET was able to detect a larger number of lesions (592 positive with 63 equivocal) than CIM (520 positive with 61 equivocal) overall, in both HNPC and CRPC patients. (18)F-DCFBC PET detection of lymph nodes, bone lesions, and visceral lesions was superior to CIM. When intrapatient clustering effects were considered, (18)F-DCFBC PET was estimated to be positive in a large proportion of lesions that would be negative or equivocal on CIM (0.45). On follow-up, the sensitivity of (18)F-DCFBC PET (0.92) was superior to CIM (0.71). (18)F-DCFBC tumor uptake was increased at the later PET time point (~2.5 h after injection), with background uptake showing a decreasing trend on later PET.
Conclusion: PET imaging with (18)F-DCFBC, a small-molecule PSMA-targeted radiotracer, detected more lesions than CIM and promises to diagnose and stage patients with metastatic prostate cancer more accurately than current imaging methods.
Keywords: bone scan; computed tomography; metastatic prostate cancer; positron emission tomography; prostate-specific membrane antigen.
© 2016 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Conflict of interest statement
Figures
Similar articles
-
¹⁸F-DCFBC PET/CT for PSMA-Based Detection and Characterization of Primary Prostate Cancer.J Nucl Med. 2015 Jul;56(7):1003-1010. doi: 10.2967/jnumed.115.154336. Epub 2015 Jun 11. J Nucl Med. 2015. PMID: 26069305 Free PMC article.
-
PSMA-Based [(18)F]DCFPyL PET/CT Is Superior to Conventional Imaging for Lesion Detection in Patients with Metastatic Prostate Cancer.Mol Imaging Biol. 2016 Jun;18(3):411-9. doi: 10.1007/s11307-016-0957-6. Mol Imaging Biol. 2016. PMID: 27080322 Free PMC article. Clinical Trial.
-
A Prospective Comparison of 18F-Sodium Fluoride PET/CT and PSMA-Targeted 18F-DCFBC PET/CT in Metastatic Prostate Cancer.J Nucl Med. 2018 Nov;59(11):1665-1671. doi: 10.2967/jnumed.117.207373. Epub 2018 Mar 30. J Nucl Med. 2018. PMID: 29602821 Free PMC article. Clinical Trial.
-
Current and potential future role of PSMA-PET in patients with castration-resistant prostate cancer.World J Urol. 2019 Mar;37(3):457-467. doi: 10.1007/s00345-018-2408-2. Epub 2018 Jul 20. World J Urol. 2019. PMID: 30030659 Review.
-
How PET-CT is Changing the Management of Non-metastatic Castration-resistant Prostate Cancer?: Comment la TEP-TDM Peut Modifier la Prise en Charge du Cancer de la Prostate Non Métastatique Résistant à la Castration ?Prog Urol. 2022 Jun;32(6S1):6S43-6S53. doi: 10.1016/S1166-7087(22)00174-9. Prog Urol. 2022. PMID: 36719646 Review.
Cited by
-
Comparison of cross-sectional imaging techniques for the detection of prostate cancer lymph node metastasis: a critical review.Transl Androl Urol. 2020 Jun;9(3):1415-1427. doi: 10.21037/tau.2020.03.20. Transl Androl Urol. 2020. PMID: 32676426 Free PMC article. Review.
-
Why Targeting PSMA Is a Game Changer in the Management of Prostate Cancer.J Nucl Med. 2018 Feb;59(2):177-182. doi: 10.2967/jnumed.117.191874. Epub 2017 Oct 6. J Nucl Med. 2018. PMID: 28986509 Free PMC article. Review.
-
PSMA-Targeted Theranostic Nanocarrier for Prostate Cancer.Theranostics. 2017 Jun 24;7(9):2477-2494. doi: 10.7150/thno.18879. eCollection 2017. Theranostics. 2017. PMID: 28744329 Free PMC article.
-
Pearls and pitfalls in clinical interpretation of prostate-specific membrane antigen (PSMA)-targeted PET imaging.Eur J Nucl Med Mol Imaging. 2017 Nov;44(12):2117-2136. doi: 10.1007/s00259-017-3780-7. Epub 2017 Aug 1. Eur J Nucl Med Mol Imaging. 2017. PMID: 28765998 Review.
-
Keeping up with the prostate-specific membrane antigens (PSMAs): an introduction to a new class of positron emission tomography (PET) imaging agents.Transl Androl Urol. 2018 Oct;7(5):831-843. doi: 10.21037/tau.2018.08.03. Transl Androl Urol. 2018. PMID: 30456186 Free PMC article. Review.
References
-
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64:9–29. - PubMed
-
- Bauman G, Belhocine T, Kovacs M, Ward A, Beheshti M, Rachinsky I. 18F-fluorocholine for prostate cancer imaging: a systematic review of the literature. Prostate Cancer Prostatic Dis. 2012;15:45–55. - PubMed
-
- Beheshti M, Treglia G, Zakavi SR, et al. Application of 11C-acetate positron-emission tomography (PET) imaging in prostate cancer: systematic review and meta-analysis of the literature. BJU Int. 2013;2013:13. - PubMed
-
- Evangelista L, Guttilla A, Zattoni F, Muzzio PC. Utility of choline positron emission tomography/computed tomography for lymph node involvement identification in intermediate- to high-risk prostate cancer: a systematic literature review and meta-analysis. Eur Urol. 2013;63:1040–1048. - PubMed
-
- Evangelista L, Zattoni F, Guttilla A, Saladini G, Colletti PM, Rubello D. Choline PET or PET/CT and biochemical relapse of prostate cancer: a systematic review and meta-analysis. Clin Nucl Med. 2013;38:305–314. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous