

Disparities in Electronic Health Record Patient Portal Use in Nephrology Clinics
- PMID: 26493242
- PMCID: PMC4633780
- DOI: 10.2215/CJN.01640215
Disparities in Electronic Health Record Patient Portal Use in Nephrology Clinics
Abstract
Background and objectives: Electronic health record (EHR) patient portals allow individuals to access their medical information with the intent of patient empowerment. However, little is known about portal use in nephrology patients. We addressed this gap by characterizing adoption of an EHR portal, assessing secular trends, and examining the association of portal adoption and BP control (<140/90 mmHg).
Design, setting, participants, & measurements: Patients seen between January 1, 2010, and December 31, 2012, at any of four university-affiliated nephrology offices who had at least one additional nephrology follow-up visit before June 30, 2013, were included. Sociodemographic characteristics, comorbidities, clinical measurements, and office visits were abstracted from the EHR. Neighborhood median household income was obtained from the American Community Survey 2012.
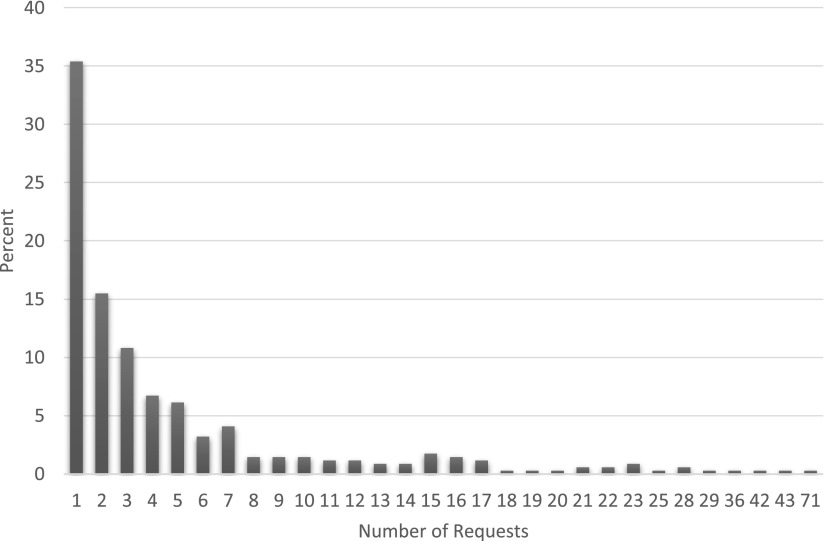
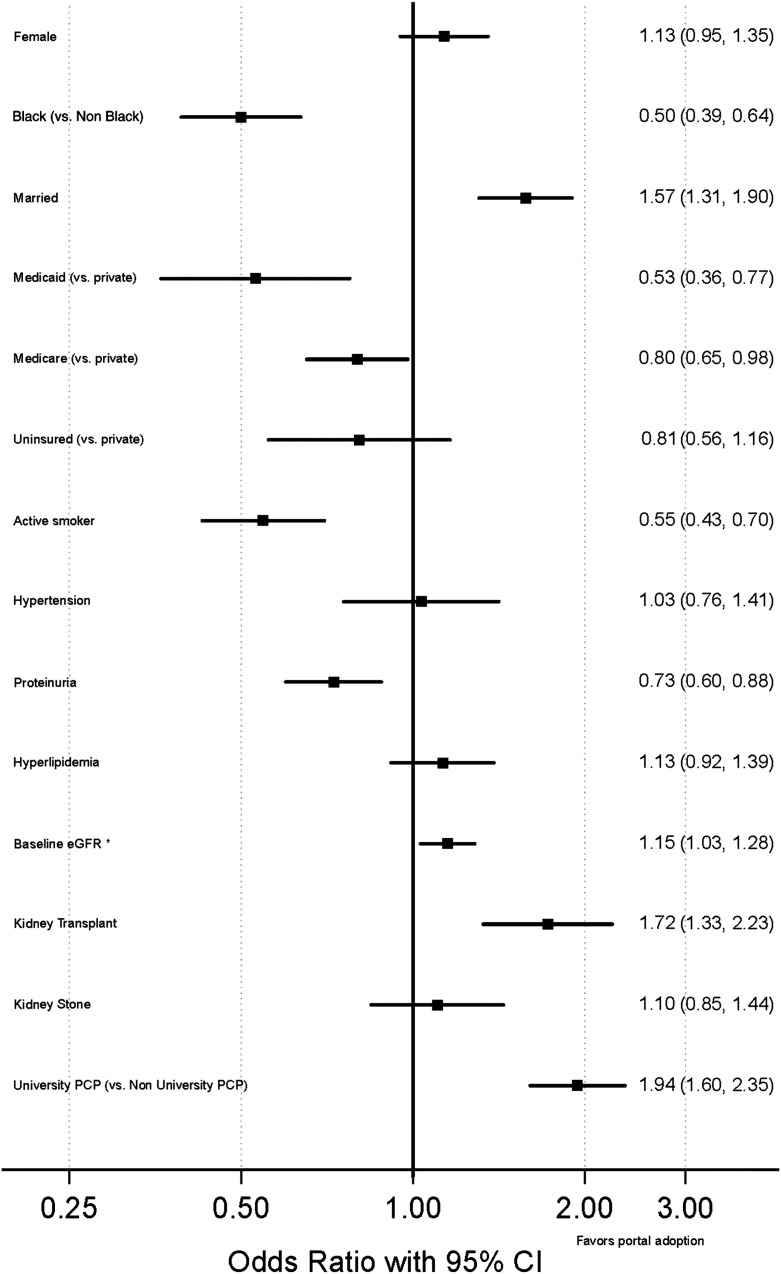
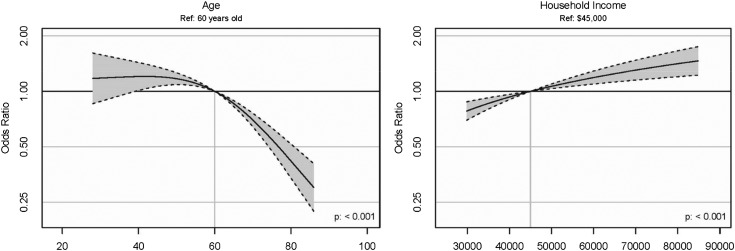
Results: Of 2803 patients, 1098 (39%) accessed the portal. Over 87% of users reviewed laboratory results, 85% reviewed their medical information (e.g., medical history), 85% reviewed or altered appointments, 77% reviewed medications, 65% requested medication refills, and 31% requested medical advice from their renal provider. In adjusted models, older age, African-American race (odds ratio [OR], 0.50; 95% confidence interval [95% CI], 0.39 to 0.64), Medicaid status (OR, 0.53; 95% CI, 0.36 to 0.77), and lower neighborhood median household income were associated with not accessing the portal. Portal adoption increased over time (2011 versus 2010: OR, 1.38 [95% CI, 1.09 to 1.75]; 2012 versus 2010: OR, 1.95 [95% CI, 1.44 to 2.64]). Portal adoption was correlated with BP control in patients with a diagnosis of hypertension; however, in the fully adjusted model this was somewhat attenuated and no longer statistically significant (OR, 1.11; 95% CI, 0.99 to 1.24).
Conclusion: While portal adoption appears to be increasing, greater attention is needed to understand why vulnerable populations do not access it. Future research should examine barriers to the use of e-health technologies in underserved patients with CKD, interventions to address them, and their potential to improve outcomes.
Keywords: chronic kidney disease; electronic health record; healthcare disparities; patient portal; personalized health record.
Copyright © 2015 by the American Society of Nephrology.
Figures
Comment in
-
Electronic Health Record Patient Portals in CKD and Hypertension Management: Meaningfully Used?Clin J Am Soc Nephrol. 2015 Nov 6;10(11):1897-9. doi: 10.2215/CJN.10070915. Epub 2015 Oct 22. Clin J Am Soc Nephrol. 2015. PMID: 26493243 Free PMC article. No abstract available.
References
-
- Xue JL, Eggers PW, Agodoa LY, Foley RN, Collins AJ: Longitudinal study of racial and ethnic differences in developing end-stage renal disease among aged medicare beneficiaries. J Am Soc Nephrol 18: 1299–1306, 2007 - PubMed
-
- Hossain MP, Goyder EC, Rigby JE, El Nahas M: CKD and poverty: A growing global challenge. Am J Kidney Dis 53: 166–174, 2009 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
