

Clinical outcome and prognostic factors for central neurocytoma: twenty year institutional experience
- PMID: 26493740
- PMCID: PMC4826306
- DOI: 10.1007/s11060-015-1959-y
Clinical outcome and prognostic factors for central neurocytoma: twenty year institutional experience
Abstract
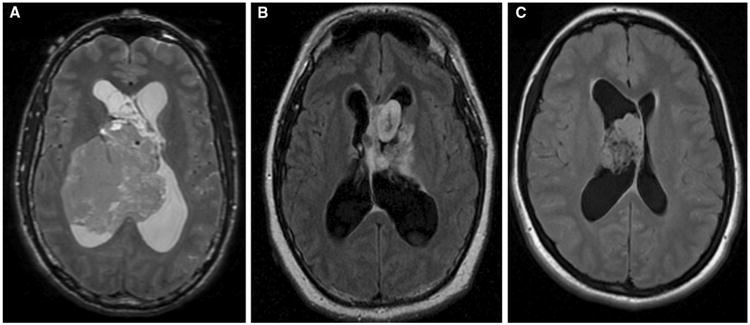
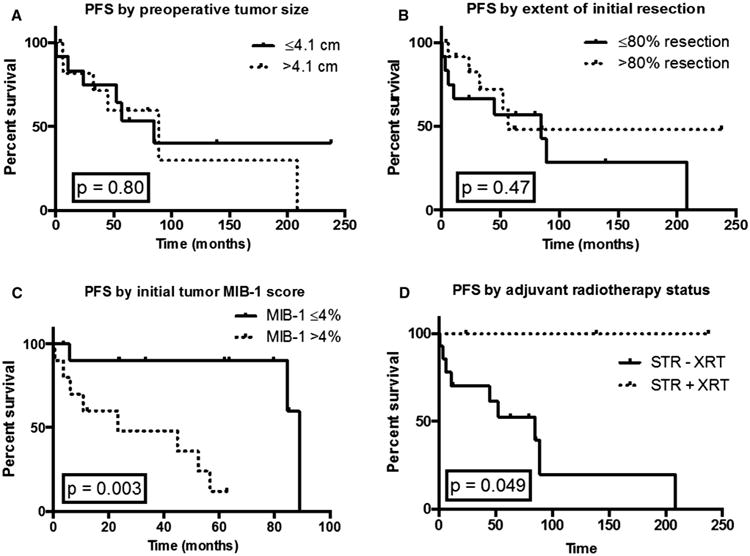
Central neurocytomas are uncommon intraventricular neoplasms whose optimal management remains controversial due to their rarity. We assessed outcomes for a historical cohort of neurocytoma patients and evaluated effects of tumor atypia, size, resection extent, and adjuvant radiotherapy. Progression-free survival (PFS) was measured by Kaplan-Meier and Cox proportional hazards methods. A total of 28 patients (15 males, 13 females) were treated between 1995 and 2014, with a median age at diagnosis of 26 years (range 5-61). Median follow-up was 62.2 months and 3 patients were lost to follow-up postoperatively. Thirteen patients experienced recurrent/progressive disease and 2-year PFS was 75% (95% CI 53-88%). Two-year PFS was 48% for MIB-1 labeling >4% versus 90% for ≤4% (HR 5.4, CI 2.2-27.8, p = 0.0026). Nine patients (32%) had gross total resections (GTR) and 19 (68%) had subtotal resections (STR). PFS for >80% resection was 83 versus 67% for ≤80% resection (HR 0.67, CI 0.23-2.0, p = 0.47). Three STR patients (16%) received adjuvant radiation which significantly improved overall PFS (p = 0.049). Estimated 5-year PFS was 67% for STR with radiotherapy versus 53% for STR without radiotherapy. Salvage therapy regimens were diverse and resulted in stable disease for 54% of patients and additional progression for 38 %. Two patients with neuropathology-confirmed atypical neurocytomas died at 4.3 and 113.4 months after initial surgery. For central neurocytomas, MIB-1 labeling index >4% is predictive of poorer outcome and our data suggest that adjuvant radiotherapy after STR may improve PFS. Most patients requiring salvage therapy will be stabilized and multiple modalities can be effectively utilized.
Conflict of interest statement
Figures
References
-
- Hassoun J, Gambarelli D, Grisoli F, Pellet W, Salamon G, Pellissier JF, Toga M. Central neurocytoma. An electron-microscopic study of two cases. Acta Neuropathol (Berl) 1982;56:151–156. - PubMed
-
- Mozes P, Szanto E, Tiszlavicz L, Barzo P, Cserhati A, Fodor E, Hideghety K. Clinical Course of Central Neurocytoma with Malignant Transformation-An Indication for Craniospinal Irradiation. Pathol Oncol Res POR 2013 - PubMed
-
- Hassoun J, Söylemezoglu F, Gambarelli D, Figarella-Branger D, von Ammon K, Kleihues P. Central neurocytoma: a synopsis of clinical and histological features. Brain Pathol Zurich Switz. 1993;3:297–306. - PubMed
-
- Sharma MC, Deb P, Sharma S, Sarkar C. Neurocytoma: a comprehensive review. Neurosurg Rev. 2006;29:270–285. - PubMed
-
- Schmidt MH, Gottfried ON, von Koch CS, Chang SM, McDermott MW. Central neurocytoma: a review. J Neurooncol. 2004;66:377–384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
