

A practical guide for performing arthrography under fluoroscopic or ultrasound guidance
- PMID: 26493836
- PMCID: PMC4656236
- DOI: 10.1007/s13244-015-0442-9
A practical guide for performing arthrography under fluoroscopic or ultrasound guidance
Abstract
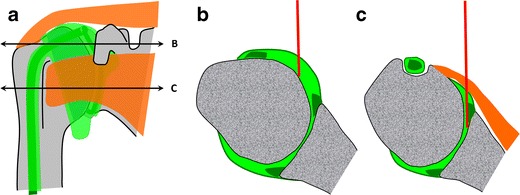
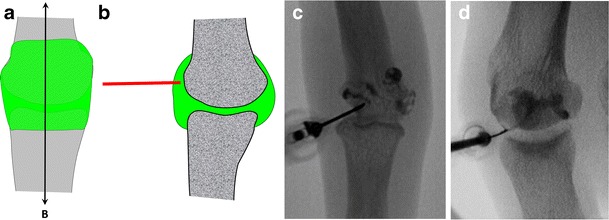
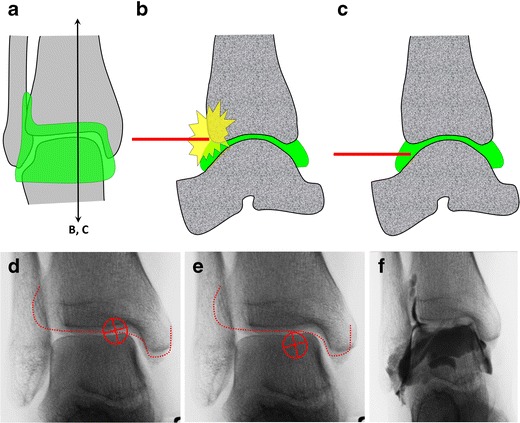
We propose a practical approach for performing arthrography with fluoroscopic or ultrasound guidance. Different approaches to the principal joints of the upper limb (shoulder, elbow, wrist and fingers), lower limb (hip, knee, ankle and foot) as well as the facet joints of the spine are discussed and illustrated with numerous drawings. Whenever possible, we emphasise the concept of targeting articular recesses, which offers many advantages over traditional techniques aiming at the joint space.
Teaching points: • Arthrography remains a foremost technique in musculoskeletal radiology • Most joints can be successfully accessed by targeting the articular recess • Targeting the recess offers several advantages over traditional approaches • Ultrasound-guidance is now favoured over fluoroscopy and targeting the recess is equally applicable.
Keywords: Arthrography; Articular recess; Fluoroscopy; Intra-articular injection; Ultrasound.
Figures















Similar articles
-
Fundamentals of Joint Injection.AJR Am J Roentgenol. 2016 Sep;207(3):484-94. doi: 10.2214/AJR.16.16243. Epub 2016 Jun 8. AJR Am J Roentgenol. 2016. PMID: 27276101 Review.
-
Ultrasound-guided joint injections for MR arthrography in pediatric patients: how we do it.Pediatr Radiol. 2015 Mar;45(3):308-16; quiz 305-7. doi: 10.1007/s00247-014-3212-9. Epub 2015 Mar 1. Pediatr Radiol. 2015. PMID: 25726013 Review.
-
Ultrasound guidance to perform intra-articular injection of gadolinium-based contrast material for magnetic resonance arthrography as an alternative to fluoroscopy: the time is now.Eur Radiol. 2016 May;26(5):1221-5. doi: 10.1007/s00330-015-3945-3. Epub 2015 Aug 8. Eur Radiol. 2016. PMID: 26253260
-
Direct MR arthrography without image guidance: a practical guide, joint-by-joint.Skeletal Radiol. 2025 Jan;54(1):17-26. doi: 10.1007/s00256-024-04709-0. Epub 2024 May 27. Skeletal Radiol. 2025. PMID: 38801542 Review.
-
Ultrasound-guided interventions of the upper extremity joints.Skeletal Radiol. 2023 May;52(5):897-909. doi: 10.1007/s00256-022-04148-9. Epub 2022 Aug 13. Skeletal Radiol. 2023. PMID: 35962837 Free PMC article. Review.
Cited by
-
Fluoroscopic-guided procedures of the lower extremity.Skeletal Radiol. 2023 May;52(5):855-874. doi: 10.1007/s00256-022-04139-w. Epub 2022 Aug 5. Skeletal Radiol. 2023. PMID: 35930079 Free PMC article. Review.
-
Pearls and pitfalls of fluoroscopic-guided foot and ankle injections: what the radiologist needs to know.Skeletal Radiol. 2019 Nov;48(11):1661-1674. doi: 10.1007/s00256-019-03226-9. Epub 2019 May 6. Skeletal Radiol. 2019. PMID: 31062056 Review.
-
Visualisation of facet joint recesses of the cadaveric spine: a micro-CT and sheet plastination study.BMJ Open Sport Exerc Med. 2018 Feb 28;4(1):e000338. doi: 10.1136/bmjsem-2017-000338. eCollection 2018. BMJ Open Sport Exerc Med. 2018. PMID: 29527323 Free PMC article.
-
Emerging role of integrated PET-MRI in osteoarthritis.Skeletal Radiol. 2021 Dec;50(12):2349-2363. doi: 10.1007/s00256-021-03847-z. Epub 2021 Jun 29. Skeletal Radiol. 2021. PMID: 34185124 Review.
-
The Posterior Transtriceps Approach for Intra-articular Elbow Arthrography: A Painless Method?Cureus. 2022 Nov 18;14(11):e31642. doi: 10.7759/cureus.31642. eCollection 2022 Nov. Cureus. 2022. PMID: 36540446 Free PMC article.
References
-
- Bonakdarpour A, Reinus WR, Khurana JS (2010) Diagnostic imaging of musculoskeletal diseases: a systematic approach. Springer, New York
LinkOut - more resources
Full Text Sources
Other Literature Sources
