

Clinical significance of donor-specific human leukocyte antigen antibodies in liver transplantation
- PMID: 26494958
- PMCID: PMC4607901
- DOI: 10.3748/wjg.v21.i39.11016
Clinical significance of donor-specific human leukocyte antigen antibodies in liver transplantation
Abstract
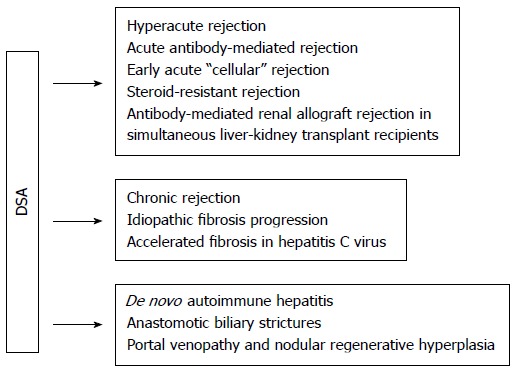
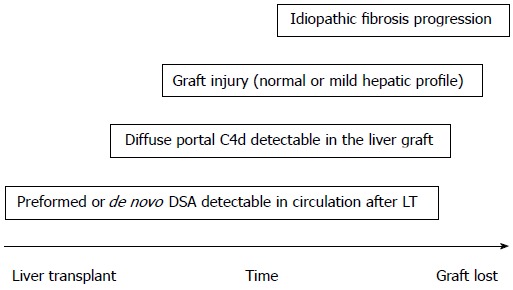
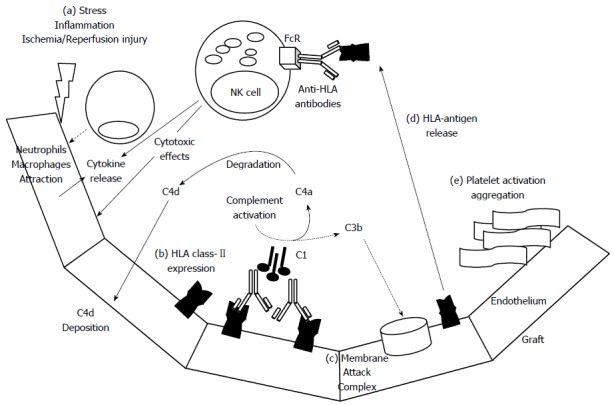
Antibody-mediated rejection (AMR) caused by donor-specific anti-human leukocyte antigen antibodies (DSA) is widely accepted to be a risk factor for decreased graft survival after kidney transplantation. This entity also plays a pathogenic role in other solid organ transplants as it appears to be an increasingly common cause of heart graft dysfunction and an emerging issue in lung transplantation. In contrast, the liver appears relatively resistant to DSA-mediated injury. This "immune-tolerance" liver property has been sustained by a low rate of liver graft loss in patients with preformed DSA and by the intrinsic liver characteristics that favor the absorption and elimination of DSA; however, alloantibody-mediated adverse consequences are increasingly being recognized, and several cases of acute AMR after ABO-compatible liver transplant (LT) have been reported. Furthermore, the availability of new solid-phase assays, allowing the detection of low titers of DSA and the refinement of objective diagnostic criteria for AMR in solid organ transplants and particularly in LT, have improved the recognition and management of this entity. A cost-effective strategy of DSA monitoring, avoidance of class II human leukocyte antigen mismatching, judicious immunosuppression attached to a higher level of clinical suspicion of AMR, particularly in cases unresponsive to conventional anti-rejection therapy, can allow a rational approach to this threat.
Keywords: Acute antibody-mediated rejection; C4d; Donor-specific anti-human leukocyte antigen antibodies; Human leukocyte antigen single antigen bead; Liver transplantation; Rejection; Solid-phase immunoassays.
Figures
Similar articles
-
Preformed complement-activating low-level donor-specific antibody predicts early antibody-mediated rejection in renal allografts.Transplantation. 2013 Jan 27;95(2):341-6. doi: 10.1097/TP.0b013e3182743cfa. Transplantation. 2013. PMID: 23197178
-
Treatment of Biopsy-Proven Acute Antibody-Mediated Rejection Using Thymoglobulin (ATG) Monotherapy and a Combination of Rituximab, Intravenous Immunoglobulin, and Plasmapheresis: Lesson Learned from Primary Experience.Clin Transpl. 2014:223-30. Clin Transpl. 2014. PMID: 26281149
-
Targeted monitoring of donor-specific HLA antibodies following renal transplantation.Clin Transpl. 2011:395-400. Clin Transpl. 2011. PMID: 22755437
-
Update on Alloantibodies in Solid Organ Transplantation.Clin Transpl. 2014:125-9. Clin Transpl. 2014. PMID: 26281136 Review.
-
The Role of Donor-Specific Antibodies in Intestinal Transplantation: Experience at the University of California Los Angeles and Literature Review.Clin Transpl. 2014:153-9. Clin Transpl. 2014. PMID: 26281140 Review.
Cited by
-
Antibody Subclass Repertoire and Graft Outcome Following Solid Organ Transplantation.Front Immunol. 2016 Oct 24;7:433. doi: 10.3389/fimmu.2016.00433. eCollection 2016. Front Immunol. 2016. PMID: 27822209 Free PMC article. Review.
-
De Novo Donor Specific Antibody and Long-Term Outcome After Liver Transplantation: A Systematic Review and Meta-Analysis.Front Immunol. 2020 Dec 23;11:613128. doi: 10.3389/fimmu.2020.613128. eCollection 2020. Front Immunol. 2020. PMID: 33424868 Free PMC article.
-
Impact of Antibodies That React With Liver Tissue and Donor-Specific Anti-HLA Antibodies in Pediatric Idiopathic Posttransplantation Hepatitis.Transplantation. 2017 May;101(5):1074-1083. doi: 10.1097/TP.0000000000001653. Transplantation. 2017. PMID: 28118175 Free PMC article.
-
Prevalence and Impact of De Novo Donor-Specific Antibodies During a Multicenter Immunosuppression Withdrawal Trial in Adult Liver Transplant Recipients.Hepatology. 2019 Mar;69(3):1273-1286. doi: 10.1002/hep.30281. Epub 2019 Feb 8. Hepatology. 2019. PMID: 30229989 Free PMC article. Clinical Trial.
-
HLA Class II-Triggered Signaling Cascades Cause Endothelial Cell Proliferation and Migration: Relevance to Antibody-Mediated Transplant Rejection.J Immunol. 2018 Apr 1;200(7):2372-2390. doi: 10.4049/jimmunol.1701259. Epub 2018 Feb 23. J Immunol. 2018. PMID: 29475988 Free PMC article.
References
-
- Morales-Buenrostro LE, Castro R, Terasaki PI. Impact of immunosuppression on HLA-antibody formation. Clin Transpl. 2006:227–240. - PubMed
-
- Taner T, Gandhi MJ, Sanderson SO, Poterucha CR, De Goey SR, Stegall MD, Heimbach JK. Prevalence, course and impact of HLA donor-specific antibodies in liver transplantation in the first year. Am J Transplant. 2012;12:1504–1510. - PubMed
-
- Chan KM, Lee CS, Wu TJ, Lee CF, Chen TC, Lee WC. Clinical perspective of acute humoral rejection after blood type-compatible liver transplantation. Transplantation. 2011;91:e29–e30. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
