

Preventable Sternocleidomastoid Muscular Atrophy after Neck Dissection
- PMID: 26495217
- PMCID: PMC4596429
- DOI: 10.1097/GOX.0000000000000457
Preventable Sternocleidomastoid Muscular Atrophy after Neck Dissection
Abstract
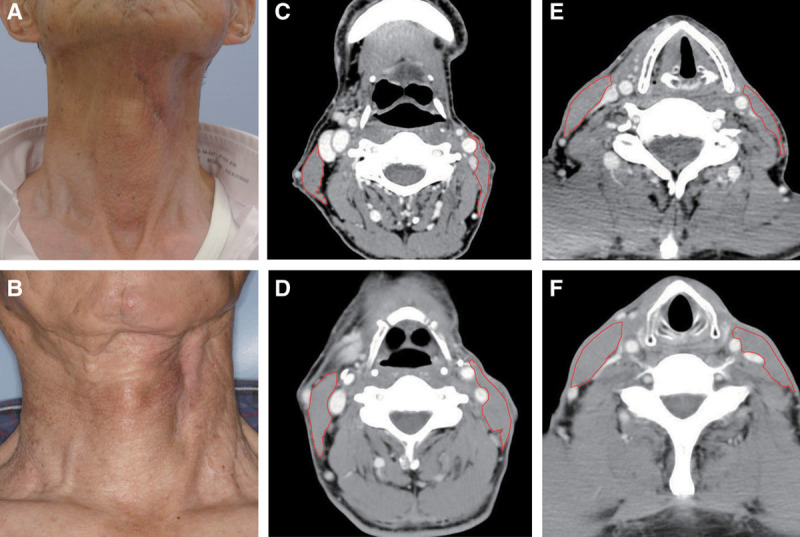
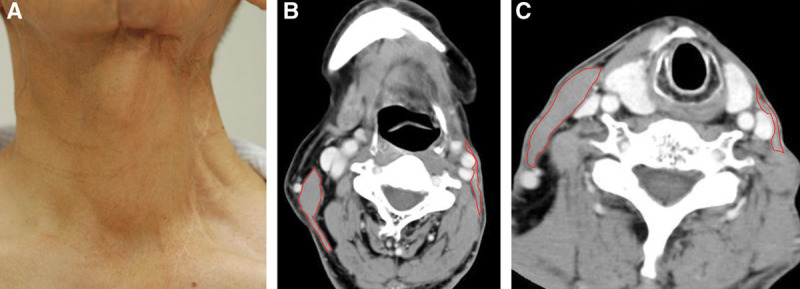
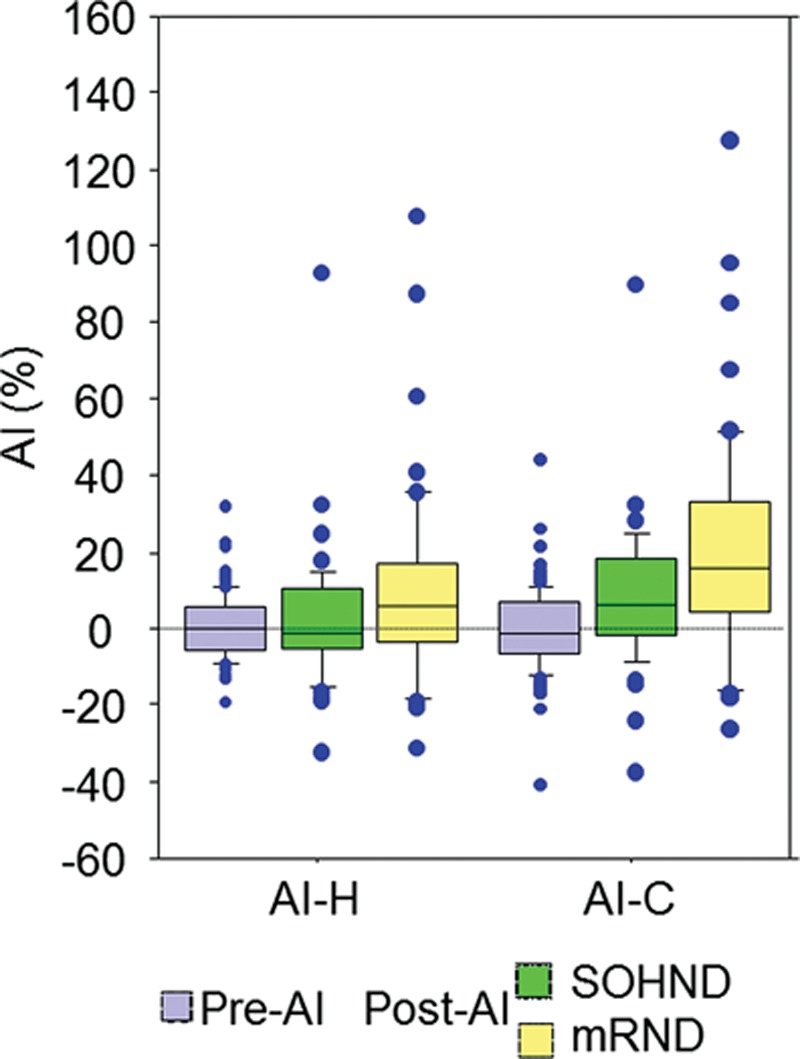
Background: Modified radical neck dissection (mRND) [preserving the sternocleidomastoid muscle (SCM) and the spinal accessory nerve] and supraomohyoid neck dissection have become common surgical procedures for treating head and neck cancer. Postoperative severe asymmetry of the neck and severe atrophy of the SCM, however, have been demonstrated.
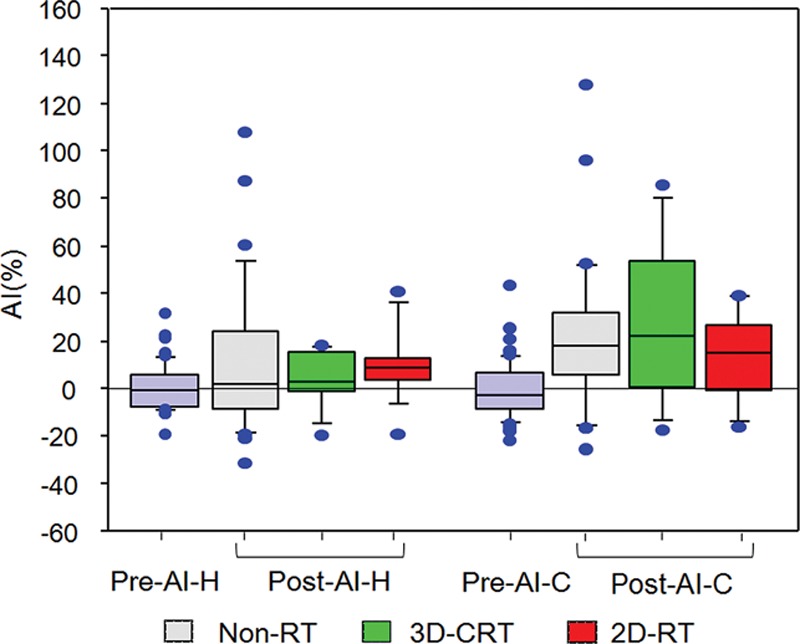
Methods: Using computed tomographic images, cross-sectional areas of the SCMs were measured in 99 patients with carcinoma of the oral cavity who underwent unilateral mRND or supraomohyoid neck dissection. An asymmetry index was used.
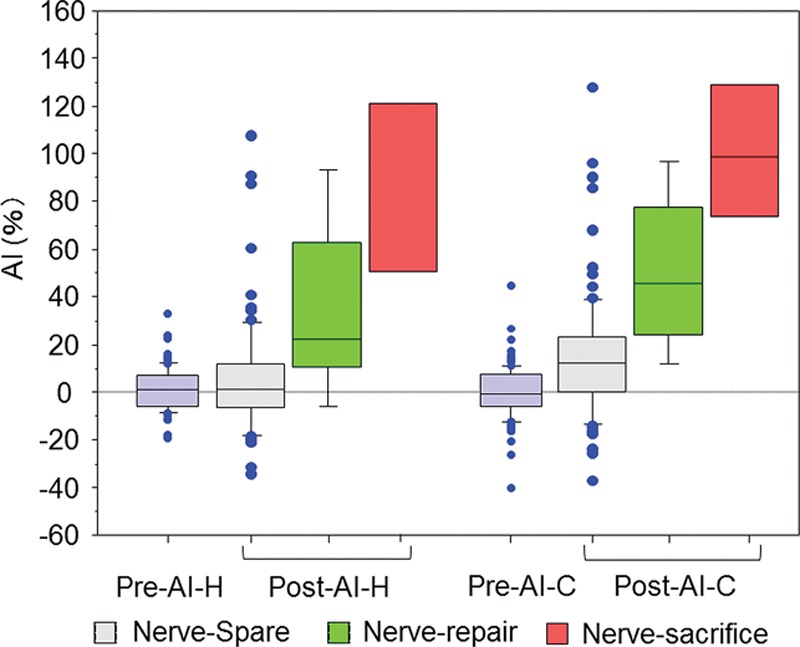
Results: Innervation to the SCM was preserved in 91 patients. The spinal accessory nerve and the innervation were sacrificed in 3 patients; the innervation was repaired in 5 patients. Sacrifice of innervation to the SCM resulted in extremely severe asymmetry. Repair of the innervation prevented severe asymmetry in 40%. Preservation of the innervation prevented severe asymmetry in 75% at the middle portion of the neck and in 56% at the lower portion after mRND.
Conclusion: Preserving innervation to the SCM and gentle handling of the nerve during neck dissection could prevent severe asymmetry after neck dissection.
Conflict of interest statement
Figures
Similar articles
-
Evidence of significant sternocleidomastoid atrophy following modified radical neck dissection type III.Plast Reconstr Surg. 2006 Jan;117(1):227-32. doi: 10.1097/01.prs.0000187150.09737.1a. Plast Reconstr Surg. 2006. PMID: 16404272
-
Identification of three anatomical patterns of the spinal accessory nerve in the neck by neurophysiological mapping.Radiol Oncol. 2014 Nov 5;48(4):387-92. doi: 10.2478/raon-2013-0069. eCollection 2014 Dec. Radiol Oncol. 2014. PMID: 25435852 Free PMC article.
-
A study of sternocleidomastoid muscular atrophy after modified neck dissection.Surg Today. 1998;28(1):46-58. doi: 10.1007/BF02483608. Surg Today. 1998. PMID: 9505317
-
Controlling advanced neck disease: efficacy of neck dissection and radiotherapy.Laryngoscope. 2000 Jul;110(7):1124-7. doi: 10.1097/00005537-200007000-00010. Laryngoscope. 2000. PMID: 10892681 Review.
-
Sternocleidomastoid muscle additionally innervated by the facial nerve: case report and review of the literature.Anat Sci Int. 2015 Jan;90(1):54-6. doi: 10.1007/s12565-013-0224-8. Epub 2013 Dec 18. Anat Sci Int. 2015. PMID: 24347311 Review.
Cited by
-
Extent of Neck Dissection and Cervical Lymph Node Involvement in Oral Squamous Cell Carcinoma.Front Oncol. 2022 May 24;12:812864. doi: 10.3389/fonc.2022.812864. eCollection 2022. Front Oncol. 2022. PMID: 35686113 Free PMC article.
-
Performance status scale for head and neck scores for oral cancer survivors: predictors and factors for improving quality of life.Clin Oral Investig. 2019 Apr;23(4):1575-1582. doi: 10.1007/s00784-018-2587-7. Epub 2018 Aug 23. Clin Oral Investig. 2019. PMID: 30141077
References
-
- Robbins KT, Clayman G, Levine PA, et al. Neck dissection classification update: revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology-Head and Neck Surgery. Archiv Otolaryngol Head Neck Surg. 2002;128:751–758. - PubMed
-
- Ahlberg A, Nikolaidis P, Engstrom T, et al. Morbidity of supraomohyoidal and modified radical neck dissection combined with radiotherapy for head and neck cancer: a prospective longitudinal study. Head Neck. 2012;34:66–72. - PubMed
-
- Cappiello J, Piazza C, Nicolai P. The spinal accessory nerve in head and neck surgery. Curr Opin Otolaryngol Head Neck Surg. 2007;15:107–111. - PubMed
-
- Orhan KS, Demirel T, Baslo B, et al. Spinal accessory nerve function after neck dissections. J Laryngol Otol. 2007;121:44–48. - PubMed
-
- Nagata T, Matsunaga K, Kawazu T, et al. Patency assessment of the internal jugular vein after neck dissection. Int J Oral Maxillofac Surg. 2006;35:416–420. - PubMed
LinkOut - more resources
Full Text Sources