

Four Principles to Consider Before Advising Women on Screening Mammography
- PMID: 26496048
- PMCID: PMC4649764
- DOI: 10.1089/jwh.2015.5220
Four Principles to Consider Before Advising Women on Screening Mammography
Abstract
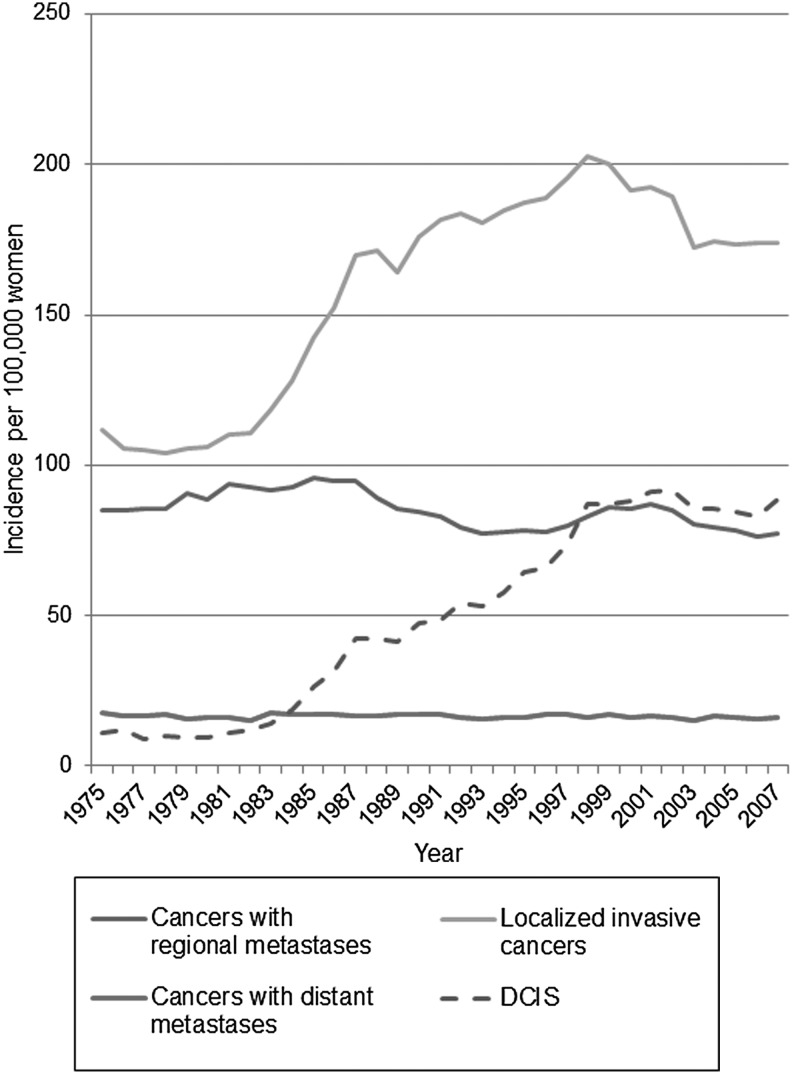
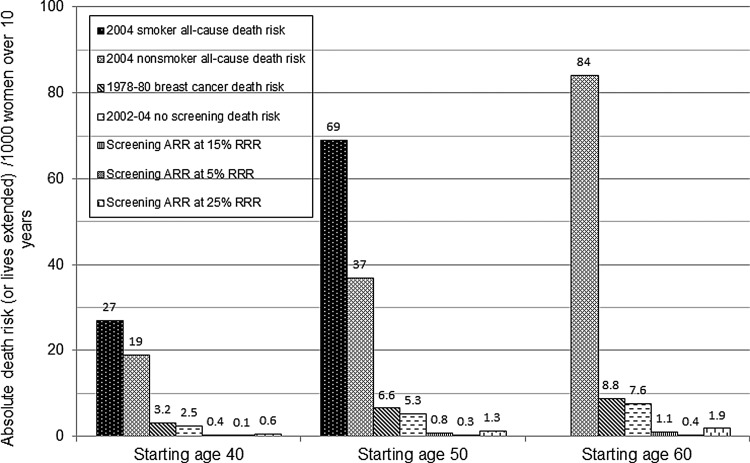
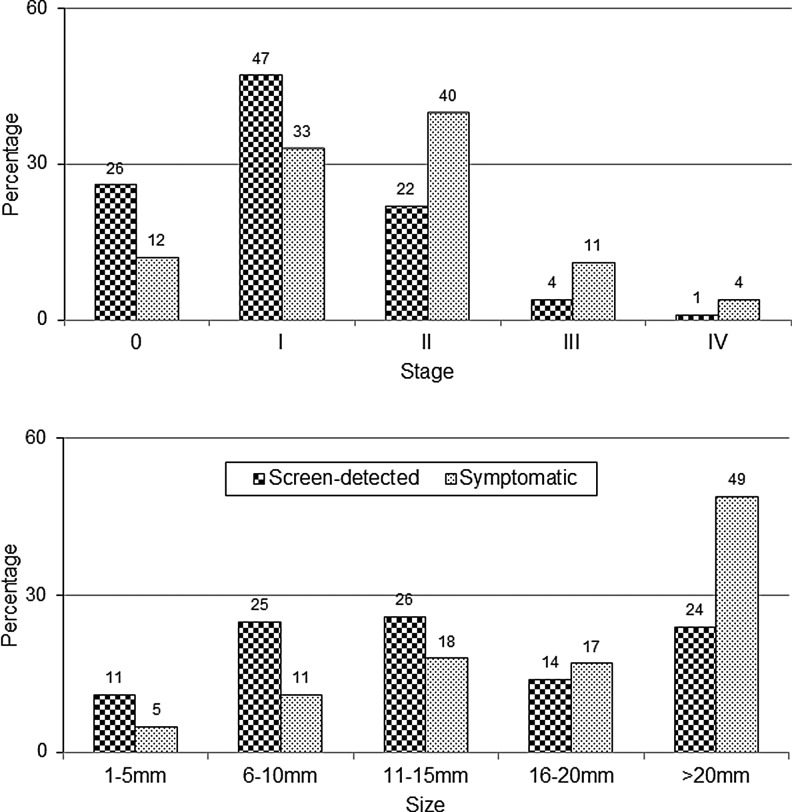
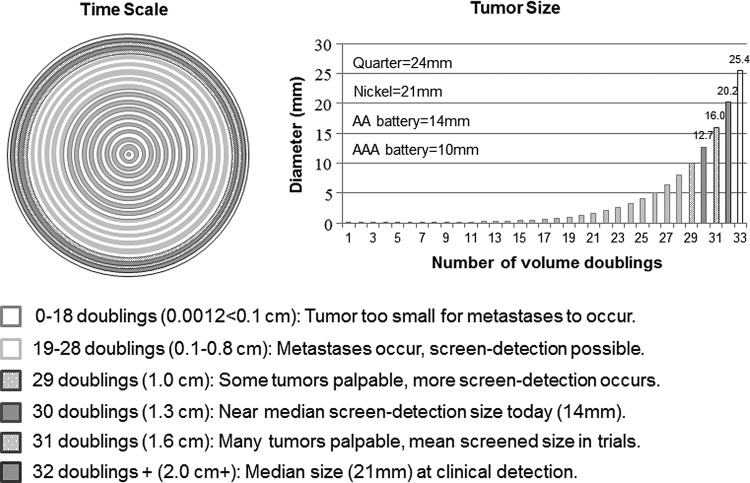
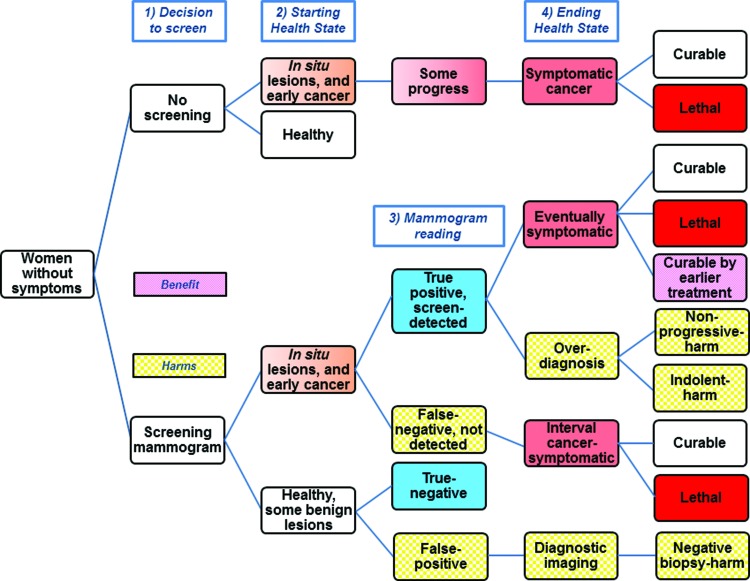
This article reviews four important screening principles applicable to screening mammography in order to facilitate informed choice. The first principle is that screening may help, hurt, or have no effect. In order to reduce mortality and mastectomy rates, screening must reduce the rate of advanced disease, which likely has not happened. Through overdiagnosis, screening produces substantial harm by increasing both lumpectomy and mastectomy rates, which offsets the often-promised benefit of less invasive therapy. Next, all-cause mortality is the most reliable way to measure the efficacy of a screening intervention. Disease-specific mortality is biased due to difficulties in attribution of cause of death and to increased mortality due to overdiagnosis and the resulting overtreatment with radiotherapy and chemotherapy. To enhance participation, the benefit from screening is often presented in relative instead of absolute terms. Third, some screening statistics must be interpreted with caution. Increased survival time and the percentage of early-stage tumors at detection sound plausible, but are affected by lead-time and length biases. In addition, analyses that only include women who attend screening cannot reliably correct for selection bias. The final principle is that accounting for tumor biology is important for accurate estimates of lead time, and the potential benefit from screening. Since "early detection" is actually late in a tumor's lifetime, the time window when screen detection might extend a woman's life is narrow, as many tumors that can form metastases will already have done so. Instead of encouraging screening mammography, physicians should help women make an informed decision as with any medical intervention.
Figures
Similar articles
-
Overdiagnosis of invasive breast cancer due to mammography screening: results from the Norwegian screening program.Ann Intern Med. 2012 Apr 3;156(7):491-9. doi: 10.7326/0003-4819-156-7-201204030-00005. Ann Intern Med. 2012. PMID: 22473436
-
Mammography screening in the county of Fyn. November 1993-December 1999.APMIS Suppl. 2003;(110):1-33. APMIS Suppl. 2003. PMID: 12739252
-
Canadian National Breast Screening Study: 2. Breast cancer detection and death rates among women aged 50 to 59 years.CMAJ. 1992 Nov 15;147(10):1477-88. CMAJ. 1992. PMID: 1423088 Free PMC article. Clinical Trial.
-
Benefits and harms of mammography screening.Breast Cancer Res. 2015 May 1;17(1):63. doi: 10.1186/s13058-015-0525-z. Breast Cancer Res. 2015. PMID: 25928287 Free PMC article. Review.
-
Breast cancer screening in the older woman: an effective way to reduce mortality?Maturitas. 2010 Jul;66(3):263-7. doi: 10.1016/j.maturitas.2010.03.016. Epub 2010 May 6. Maturitas. 2010. PMID: 20451335 Review.
Cited by
-
Factors associated with false-positive mammography at first screen in an Asian population.PLoS One. 2019 Mar 11;14(3):e0213615. doi: 10.1371/journal.pone.0213615. eCollection 2019. PLoS One. 2019. PMID: 30856210 Free PMC article.
-
Screening for reducing morbidity and mortality in malignant melanoma.Cochrane Database Syst Rev. 2019 Jun 3;6(6):CD012352. doi: 10.1002/14651858.CD012352.pub2. Cochrane Database Syst Rev. 2019. PMID: 31157404 Free PMC article.
-
Intra-urban spatial variability of breast and cervical cancer mortality in the city of São Paulo: analysis of associated factors.Rev Bras Epidemiol. 2023 Jan 9;26:e230008. doi: 10.1590/1980-549720230008.2. eCollection 2023. Rev Bras Epidemiol. 2023. PMID: 36629620 Free PMC article.
-
Massive Endoscopic Screening for Esophageal and Gastric Cancers in a High-Risk Area of China.PLoS One. 2015 Dec 23;10(12):e0145097. doi: 10.1371/journal.pone.0145097. eCollection 2015. PLoS One. 2015. PMID: 26699332 Free PMC article.
-
Breast cancer mortality and associated factors in São Paulo State, Brazil: an ecological analysis.BMJ Open. 2017 Aug 23;7(8):e016395. doi: 10.1136/bmjopen-2017-016395. BMJ Open. 2017. PMID: 28838894 Free PMC article.
References
-
- Moyer VA. What we don't know can hurt our patients: Physician innumeracy and overuse of screening tests. Ann Intern Med 2012;156:392–393 - PubMed
-
- Keen JD. Promoting screening mammography: Insight or uptake? J Am Board Fam Med 2010;23:775–782 - PubMed
-
- Berlin L. Point: Mammography, breast cancer, and overdiagnosis: The truth versus the whole truth versus nothing but the truth. J Am Coll Radiol 2014;11:642–647 - PubMed
-
- Kalager M, Adami HO, Bretthauer M. Too much mammography. BMJ 2014;348:g1403. - PubMed
-
- Stefanek ME. Uninformed compliance or informed choice? A needed shift in our approach to cancer screening. J Natl Cancer Inst 2011;103:1821–1826 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical