

Diagnostic Accuracy of APRI, AAR, FIB-4, FI, King, Lok, Forns, and FibroIndex Scores in Predicting the Presence of Esophageal Varices in Liver Cirrhosis: A Systematic Review and Meta-Analysis
- PMID: 26496312
- PMCID: PMC4620760
- DOI: 10.1097/MD.0000000000001795
Diagnostic Accuracy of APRI, AAR, FIB-4, FI, King, Lok, Forns, and FibroIndex Scores in Predicting the Presence of Esophageal Varices in Liver Cirrhosis: A Systematic Review and Meta-Analysis
Erratum in
- Medicine (Baltimore). 2016 Feb;95(5):1
-
Erratum: Diagnostic Accuracy of APRI, AAR, FIB-4, FI, King, Lok, Forns, and FibroIndex Scores in Predicting the Presence of Esophageal Varices in Liver Cirrhosis: A Systematic Review and Meta-Analysis: Erratum.Medicine (Baltimore). 2016 Feb 8;95(5):e615b. doi: 10.1097/01.md.0000480464.27661.5b. eCollection 2016 Feb. Medicine (Baltimore). 2016. PMID: 31265675 Free PMC article.
Abstract
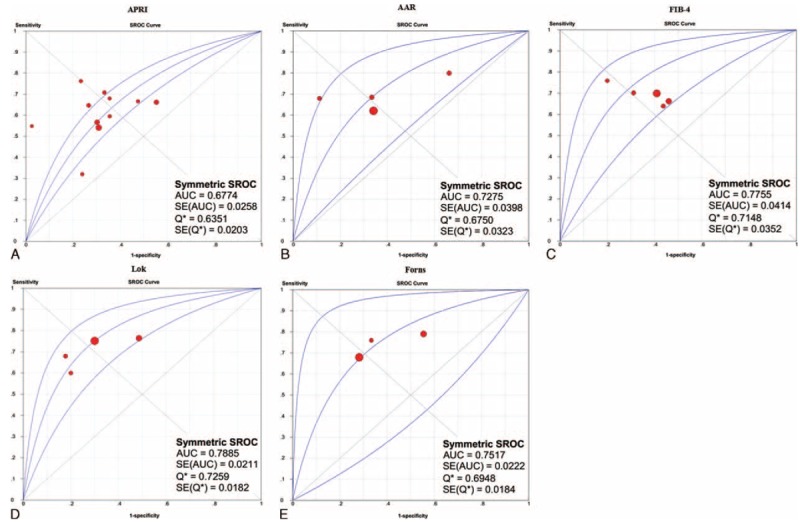
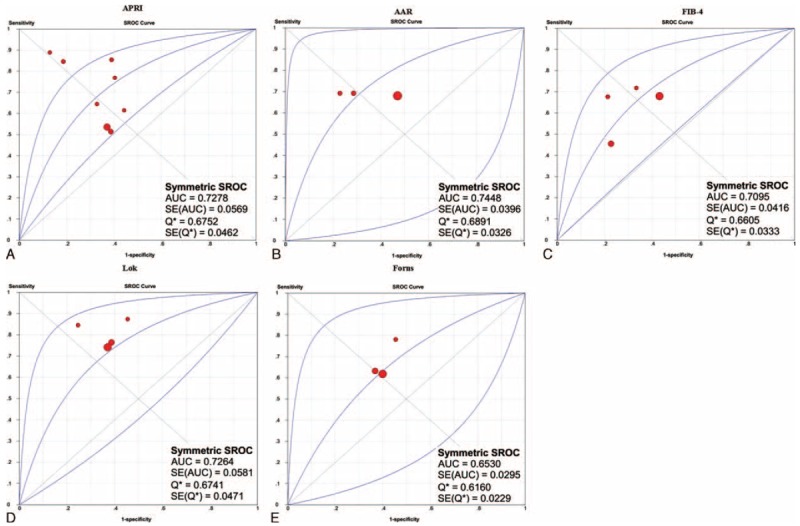
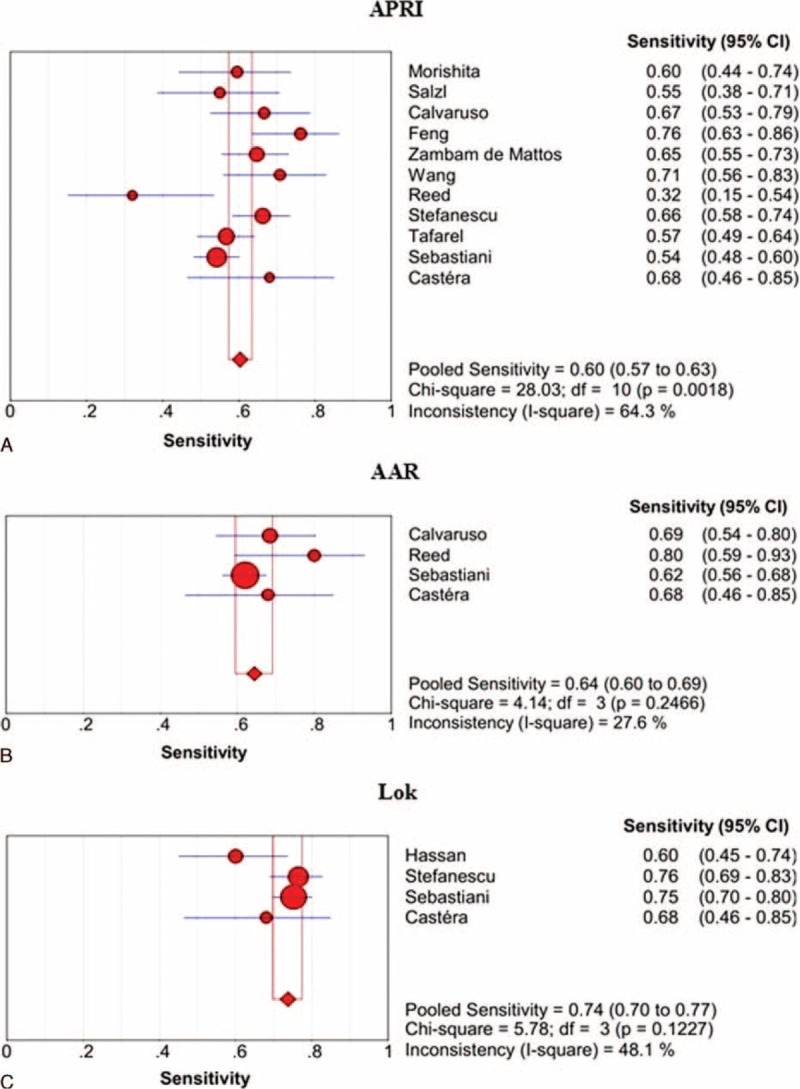
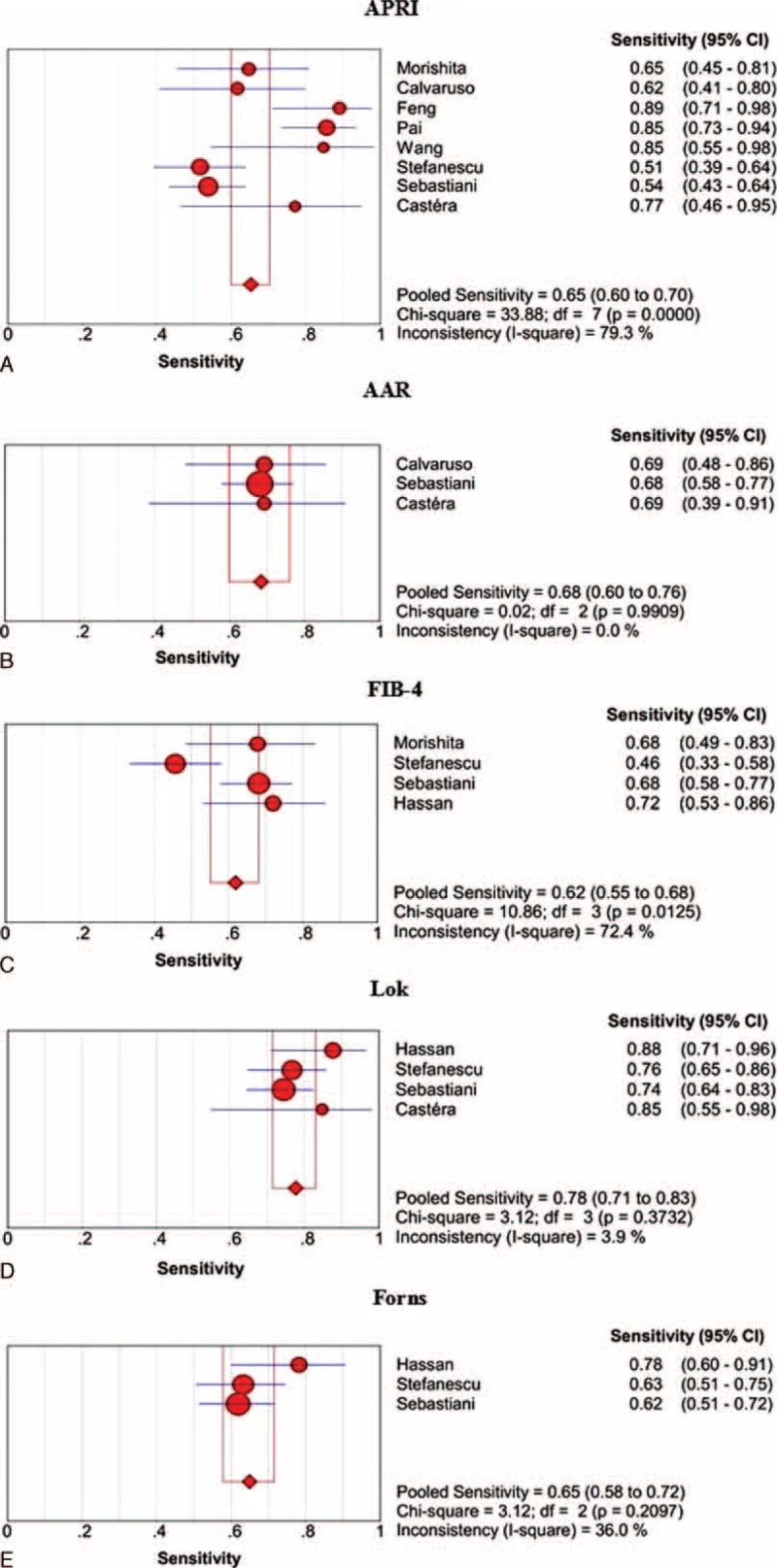
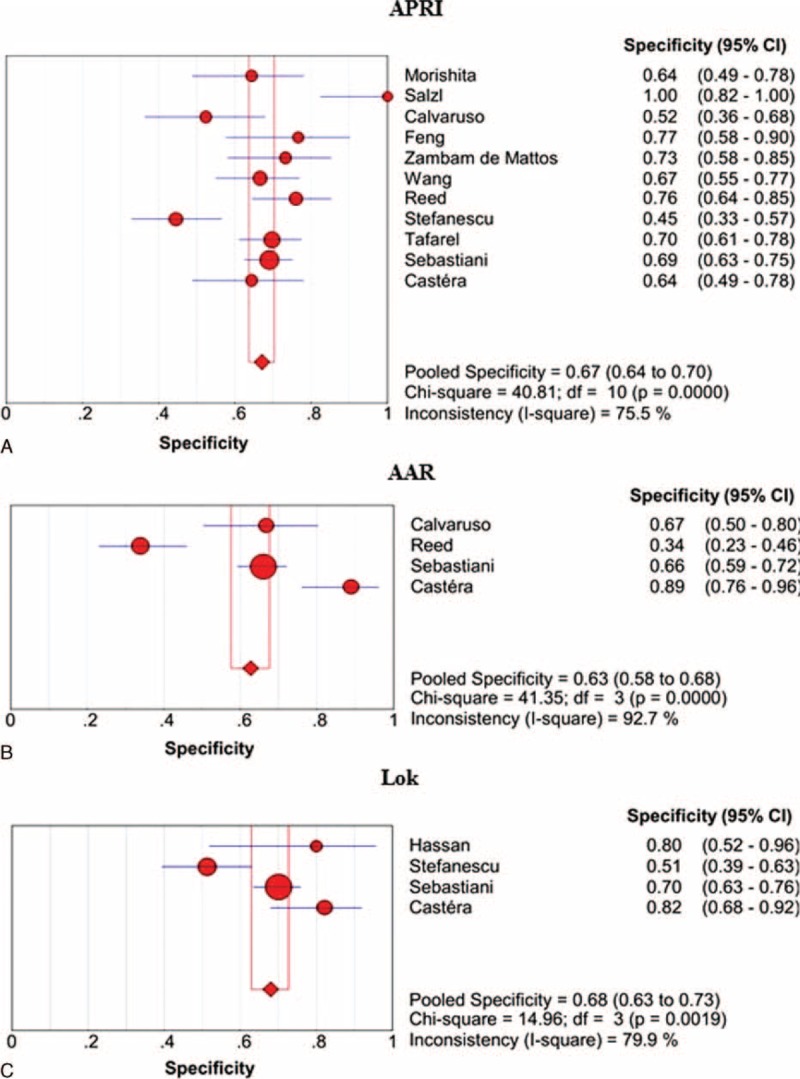
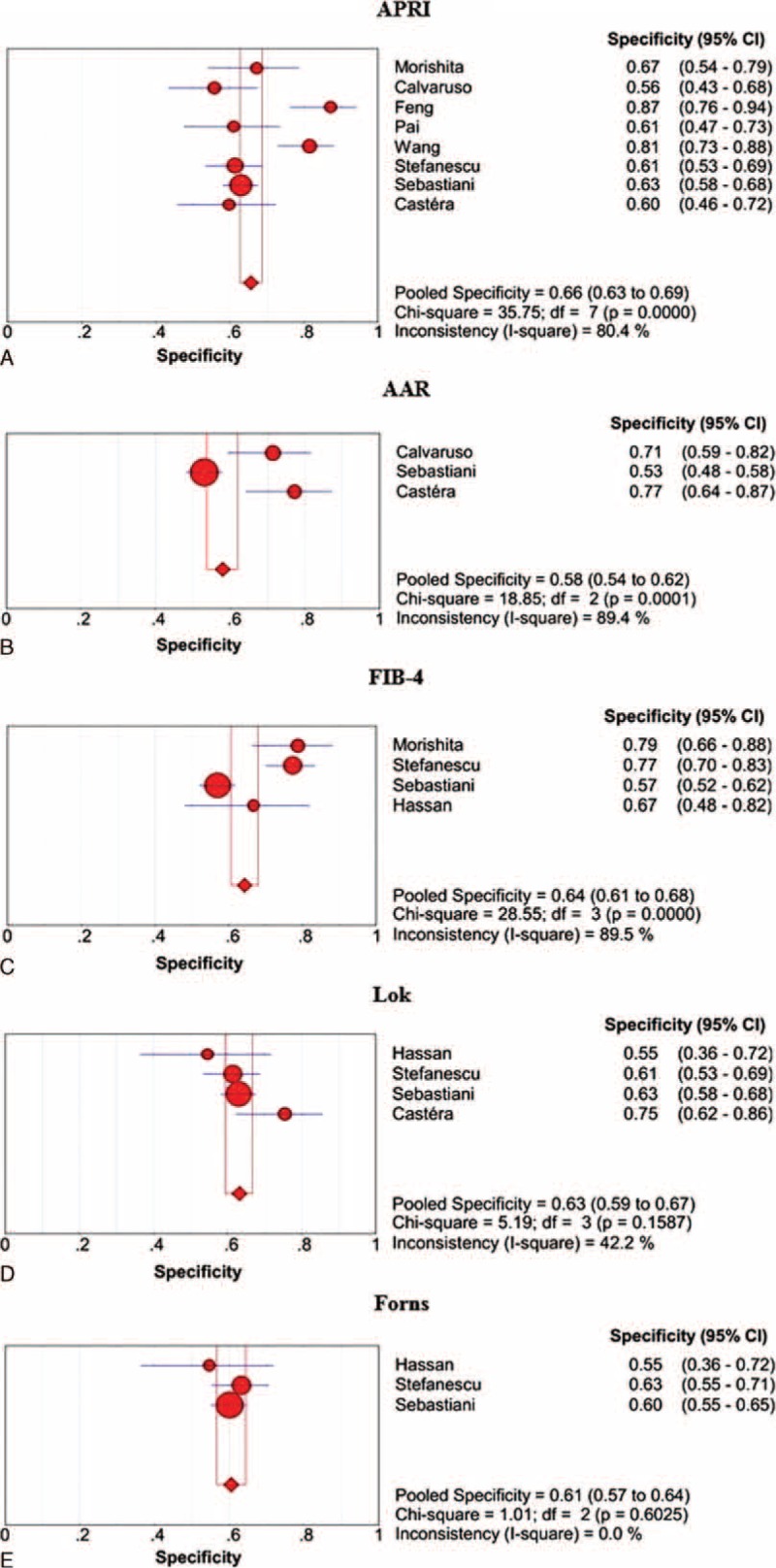
Aspartate aminotransferase-to-platelet ratio (APRI), aspartate aminotransferase-to-alanine aminotransferase ratio (AAR), FIB-4, FI, King, Lok, Forns, and FibroIndex scores may be simple and convenient noninvasive diagnostic tests, because they are based on the regular laboratory tests and demographic data. This study aimed to systematically evaluate their diagnostic accuracy for the prediction of varices in liver cirrhosis.All relevant papers were searched via PubMed, EMBASE, CNKI, and Wanfang databases. The area under the summary receiver operating characteristic curve (AUSROC), sensitivity, specificity, positive and negative likelihood ratio (PLR and NLR), and diagnostic odds ratio (DOR) were calculated.Overall, 12, 4, 5, 0, 0, 4, 3, and 1 paper was identified to explore the diagnostic accuracy of APRI, AAR, FIB-4, FI, King, Lok, Forns, and FibroIndex scores, respectively. The AUSROCs of APRI, AAR, FIB-4, Lok, and Forns scores for the prediction of varices were 0.6774, 0.7275, 0.7755, 0.7885, and 0.7517, respectively; and those for the prediction of large varices were 0.7278, 0.7448, 0.7095, 0.7264, and 0.6530, respectively. The diagnostic threshold effects of FIB-4 and Forns scores for the prediction of varices were statistically significant. The sensitivities/specificities/PLRs/NLRs/DORs of APRI, AAR, and Lok scores for the prediction of varices were 0.60/0.67/1.77/0.58/3.13, 0.64/0.63/1.97/0.54/4.18, and 0.74/0.68/2.34/0.40/5.76, respectively. The sensitivities/specificities/PLRs/NLRs/DORs of APRI, AAR, FIB-4, Lok, and Forns scores for the prediction of large varices were 0.65/0.66/2.15/0.47/4.97, 0.68/0.58/2.07/0.54/3.93, 0.62/0.64/2.02/0.56/3.57, 0.78/0.63/2.09/0.37/5.55, and 0.65/0.61/1.62/0.59/2.75, respectively.APRI, AAR, FIB-4, Lok, and Forns scores had low to moderate diagnostic accuracy in predicting the presence of varices in liver cirrhosis.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Turon F, Casu S, Hernandez-Gea V, et al. Variceal and other portal hypertension related bleeding. Best Pract Res Clin Gastroenterol 2013; 27:649–664. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
