

Midline shift in relation to thickness of traumatic acute subdural hematoma predicts mortality
- PMID: 26496765
- PMCID: PMC4620003
- DOI: 10.1186/s12883-015-0479-x
Midline shift in relation to thickness of traumatic acute subdural hematoma predicts mortality
Abstract
Background: Traumatic acute subdural hematoma has a high mortality despite intensive treatment. Despite the existence of several prediction models, it is very hard to predict an outcome. We investigated whether a specific combination of initial head CT-scan findings is a factor in predicting outcome, especially non-survival.
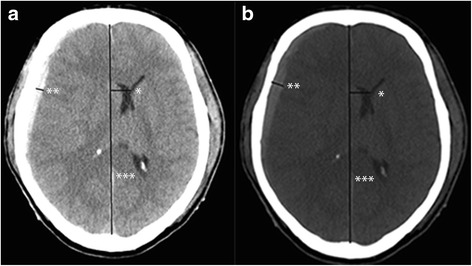
Methods: We retrospectively studied admission head CT scans of all adult patients referred for a traumatic acute subdural hematoma between April 2009 and April 2013. Chart review was performed for every included patient. Midline shift and thickness of the hematoma were measured by two independent observers. The difference between midline shift and thickness of the hematoma was calculated. These differences were correlated with outcome. IRB has approved the study.
Results: A total of 59 patients were included, of whom 29 died. We found a strong correlation between a midline shift exceeding the thickness of the hematoma by 3 mm or more, and subsequent mortality. For each evaluation, specificity was 1.0 (95 % CI: 0.85-1 for all evaluations), positive predictive value 1.0 (95 % CI between 0.31-1 and 0.56-1), while sensitivity ranged from 0.1 to 0.23 (95 % CI between 0.08-0.39 and 0.17-0.43), and negative predictive value varied from 0.52 to 0.56 (95 % CI between 0.38-0.65 and 0.41-0.69).
Conclusions: In case of a traumatic acute subdural hematoma, a difference between the midline shift and the thickness of the hematoma ≥ 3 mm at the initial CT predicted mortality in all cases. This is the first time that such a strong correlation was reported. Especially for the future development of prediction models, the relation between midline shift and thickness of the hematoma could be included as a separate factor.
Figures
References
-
- Hukkelhoven CW, Steyerberg EW, Habbema JD, Farace E, Marmarou A, Murray GD, Marshall LF, Maas AI. Predicting outcome after traumatic brain injury: development and validation of a prognostic score based on admission characteristics. J Neurotrauma. 2005;22(10):1025–1039. doi: 10.1089/neu.2005.22.1025. - DOI - PubMed
-
- Mushkudiani NA, Hukkelhoven CW, Hernandez AV, Murray GD, Choi SC, Maas AI, Steyerberg EW. A systematic review finds methodological improvements necessary for prognostic models in determining traumatic brain injury outcomes. J Clin Epidemiol. 2008;61(4):331–343. doi: 10.1016/j.jclinepi.2007.06.011. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
