

Trends and outcomes in the utilization of laparoscopic appendectomies in a low-income population in Taiwan from 2003 to 2011
- PMID: 26496832
- PMCID: PMC4619494
- DOI: 10.1186/s12939-015-0248-x
Trends and outcomes in the utilization of laparoscopic appendectomies in a low-income population in Taiwan from 2003 to 2011
Abstract
Background: Numerous epidemiological studies have compared outcomes between laparoscopic appendectomies (LA) and open appendectomies (OA); however, few studies have assessed the efficacy of LA specifically in a low-income population (LIP).
Methods: We analyzed the trends in the utilization and outcomes of LA versus OA in an LIP in Taiwan using data from the National Health Insurance (NHI) Research Database.
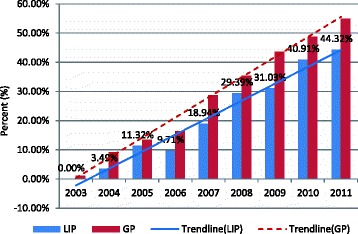
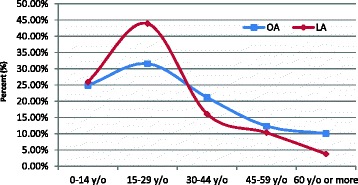
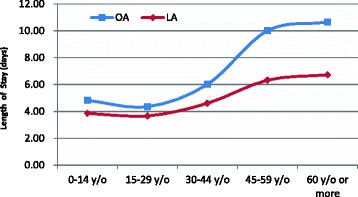
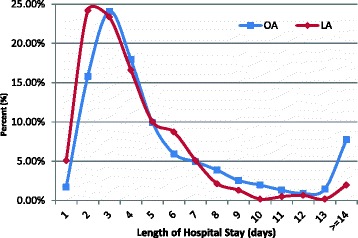
Results: Steady temporal growth trends were observed for the patients who underwent LA in both the LIP and general population (GP); however, in each study year, the proportion of LIP patients who underwent LA was lower than the proportion of GP patients who underwent the procedure. The LIP patients were more susceptible to payment policies than the GP patients; thus, more attention should be paid to vulnerable patient populations when formulating and revising NHI payment policies. Compared with OAs, LAs were associated with a slightly higher rate of routine patient discharges and a lower rate of in-hospital complications (1.48% vs. 3.76%, p < 0.05). The rate of readmission for complications was lower in patients after LA than in patients after OA (1.64% vs. 3.89%, p < 0.05). The overall case-fatality rate of LIP patients who underwent LA was lower than that of those who underwent OA. LA was correlated with a significantly shorter length of hospital stay (LOS) compared with OA (3.80 ± 0.08 vs. 5.51 ± 0.11, p < 0.05). The average hospital cost for LA was slightly less than that for OA (1178 ± 13 vs. 1191 ± 19 USD, p < 0.05). A higher percentage of patients who underwent OA required an LOS longer than 14 days compared to patients who underwent LA (7.73% vs. 1.97%, p < 0.05). Regarding hospital costs and LOS, LA showed significant advantages over OA in the subpopulations of male patients, patients 45 years old and older, patients with Charlson Comorbidity Index (CCI) scores of two or more, and patients with complicated cases of appendicitis.
Conclusion: The LIP patients benefited more from the LA approach than the OA approach in the treatment of appendicitis, especially regarding LOS, in-hospital complications, in-hospital mortality, and routine discharge rates.
Figures

References
-
- Department of Statistics (DOS), Ministry of the Interior, Survey of living conditions of low-income households in Taiwan-fuchien area (2008). http://www.mohw.gov.tw/cht/DOS/Statistic.aspx?f_list_no=312&fod_list_no=.... Accessed 5 Feb 2015.
-
- Chou Y, Lin S. Report of the survey of the basic needs for low-income families in Taoyuan county, Taiwan. Taiwan: Hsuan Chuang University; 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
