

Effectiveness of Simeprevir Plus Sofosbuvir, With or Without Ribavirin, in Real-World Patients With HCV Genotype 1 Infection
- PMID: 26497081
- PMCID: PMC4727992
- DOI: 10.1053/j.gastro.2015.10.013
Effectiveness of Simeprevir Plus Sofosbuvir, With or Without Ribavirin, in Real-World Patients With HCV Genotype 1 Infection
Abstract
Background & aims: The interferon-free regimen of simeprevir plus sofosbuvir was recommended by professional guidelines for certain patients with hepatitis C virus (HCV) genotype 1 infection based on the findings of a phase 2 trial. We aimed to evaluate the safety and efficacy of this regimen in clinical practice settings in North America.
Methods: We collected demographic, clinical, and virologic data, as well as reports of adverse outcomes, from sequential participants in HCV-TARGET--a prospective observational cohort study of patients undergoing HCV treatment in routine clinical care settings. From January through October 2014, there were 836 patients with HCV genotype 1 infection who began 12 weeks of treatment with simeprevir plus sofosbuvir (treatment duration of up to 16 weeks); 169 of these patients received ribavirin. Most patients were male (61%), Caucasian (76%), or black (13%); 59% had cirrhosis. Most patients had failed prior treatment with peginterferon and ribavirin without (46%) or with telaprevir or boceprevir (12%). The primary outcome was sustained virologic response (SVR), defined as the level of HCV RNA below quantification at least 64 days after the end of treatment (beginning of week 12 after treatment--a 2-week window). Logistic regression models with inverse probability weights were constructed to adjust for baseline covariates and potential selection bias.
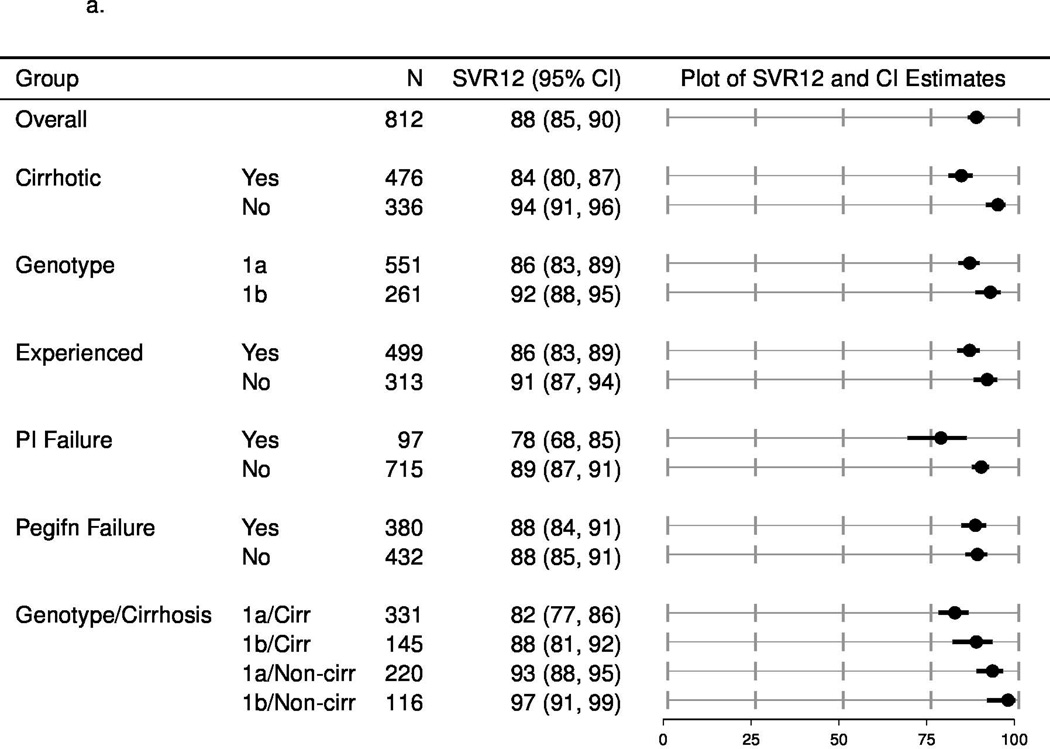
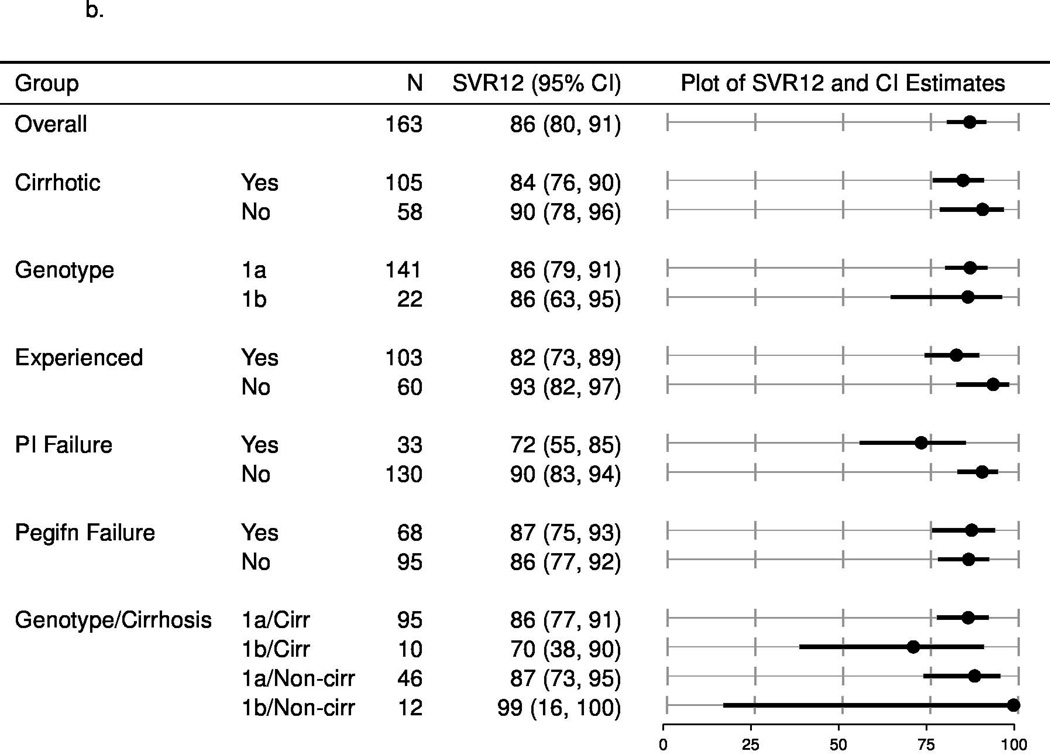
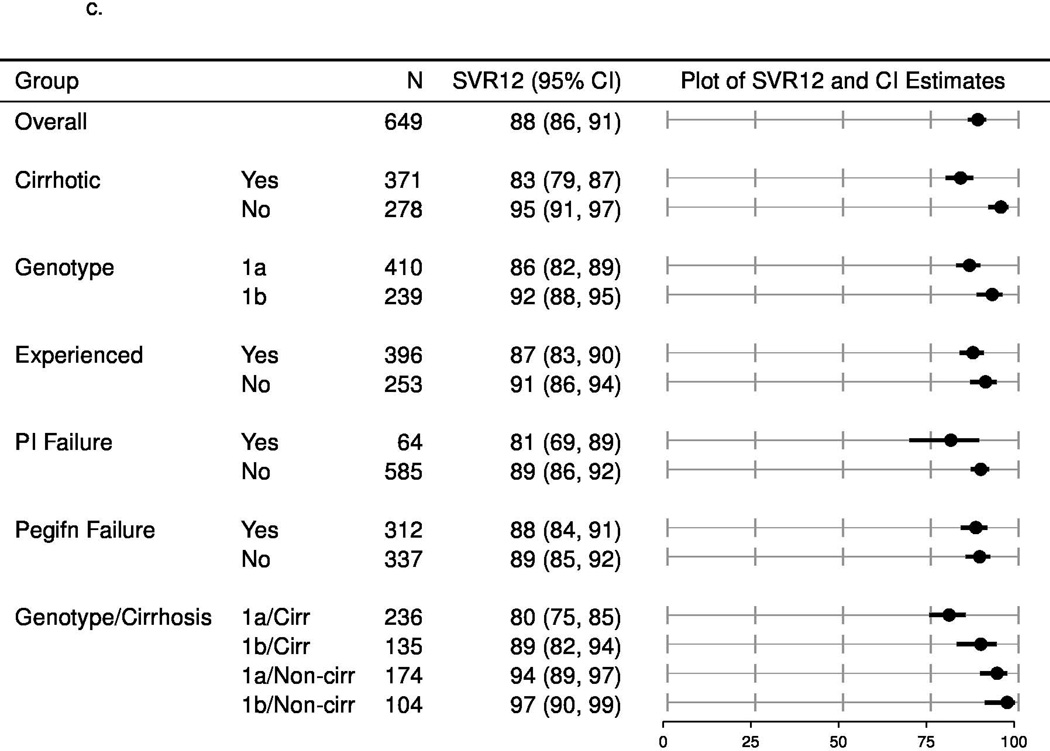
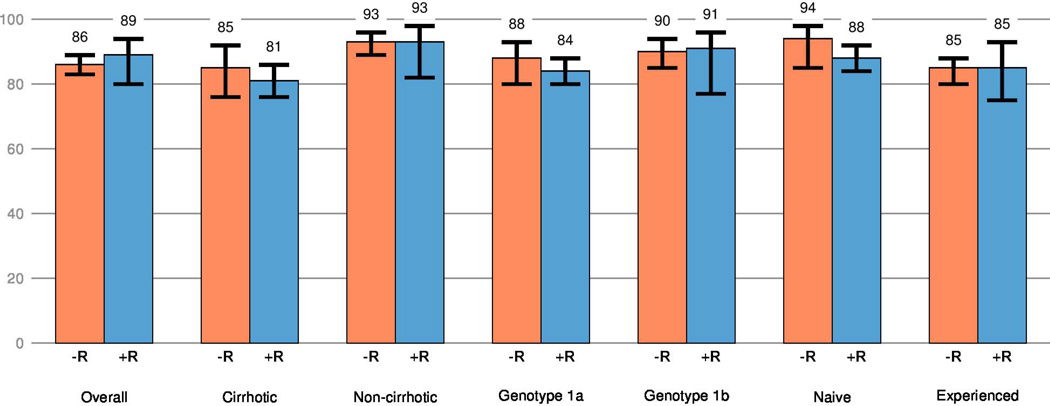
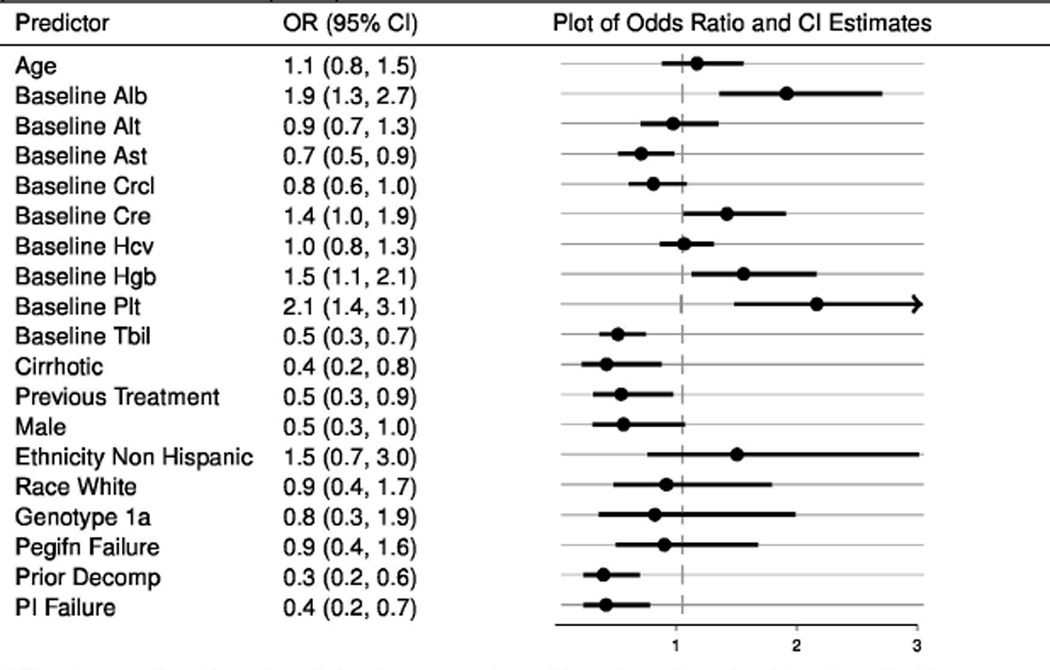
Results: The overall SVR rate was 84% (675 of 802 patients, 95% confidence interval, 81%-87%). Model-adjusted estimates indicate patients with cirrhosis, prior decompensation, and previous protease inhibitor treatments were less likely to achieve an SVR. The addition of ribavirin had no detectable effects on SVR. The most common adverse events were fatigue, headache, nausea, rash, and insomnia. Serious adverse events and treatment discontinuation occurred in only 5% and 3% of participants, respectively.
Conclusions: In a large prospective observational cohort study, a 12-week regimen of simeprevir plus sofosbuvir was associated with high rates of SVR and infrequent treatment discontinuation. ClinicalTrials.gov: NCT01474811.
Keywords: Chronic Hepatitis; Direct-Acting Agent; NS3/4A Protease Inhibitor; NS5B.
Copyright © 2016 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Sulkowski reports grants and personal fees from Gilead, grants and personal fees from Janssen, during the conduct of the study; personal fees from Achillion, grants and personal fees from AbbVie, grants and personal fees from Merck, grants and personal fees from BMS, outside the submitted work.
Dr. Vargas reports grant funding from AbbVie, Gilead, Merck, and BMS during the conduct of the study.
Dr. Di Bisceglie reports grant funding from Gilead, AbbVie, Janssen during the conduct of the study; consultant funds from Gilead and AbbVie outside the submitted work.
Dr. Kuo reports grant funding from Gilead during the conduct of the study.
Dr. Reddy reports grant funding from AbbVie, Merck, Gilead, Janssen and Vertex during the conduct of the study.
Dr. Lim reports grant funding from AbbVie, Achillion, Bohringer-Ingelheim, Bristol-Myers Squibb, Gilead, Glaxo-Smith Kline, Janssen, and Vertex during the conduct of the study; consultant funds from Boehringer-Ingelheim, Bristol-Myers Squibb, Gilead, Janssen, and Merck.
Dr. Morelli reports grant funding from AbbVie, BMS, Gilead, Merck, Janssen, Vertex, Idenix, Conatus, and Salix during the conduct of the study.
Dr. Darling reports grant funding from Bristol-Myers Squibb during the conduct of the study.
Dr. Feld reports grant funding from AbbVie, Boehringer-Ingelheim, Gilead, Janssen, Merck, and Santaris during the conduct of the study.
Dr. Brown reports grant and consultant funding from Gilead and Janssen during the conduct of the study.
Lynn Frazier, ARNP reports grant and consultant funding from AbbVie, Gilead, Janssen, and Merck during the conduct of the study.
Thomas G. Stewart, MS reports no disclosures during the conduct of the study.
Dr. Fried reports grant funding from AbbVie, Bristol-Myers Squibb, Gilead, Glaxo, Merck, Vertex, Genentech/Roche and consultant funding from Genentech/Roche, Tibotec/Janssen, Vertex, Merck, Glaxo, Novartis, AbbVie, Gilead, Bristol-Myers Squibb during the conduct of the study along with funding from the NIH for research.
Dr. Nelson reports grant funding from AbbVie, Gilead, BMS, Janssen, Merck, Vertex, and GSK during the conduct of the study.
Dr. Jacobson reports grant funding from AbbVie, BMS, Gilead, Janssen, Merck, and Tobira during the conduct of the study. He reports consultant and advisor funding from AbbVie, Achillion, Alnylam, BMS, Enanta, Gilead, Janssen, Merck during the time of the study. He also reports funding from AbbVie, BMS, Gilead, and Janssen for Speakers’ Bureau.
Figures
References
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, et al. Global epidemiology of hepatitis C virus infection: new estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57:1333–1342. - PubMed
-
- Backus LI, Boothroyd DB, Phillips BR, et al. A sustained virologic response reduces risk of all-cause mortality in patients with hepatitis C. Clin.Gastroenterol.Hepatol. 2011;9:509–516. - PubMed
-
- van der Meer AJ, Veldt BJ, Feld JJ, et al. Association between sustained virological response and all-cause mortality among patients with chronic hepatitis C and advanced hepatic fibrosis. JAMA. 2012;308:2584–2593. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
