

Assessing and monitoring intratumor heterogeneity in glioblastoma: how far has multimodal imaging come?
- PMID: 26497327
- PMCID: PMC6083939
- DOI: 10.2217/cns.15.20
Assessing and monitoring intratumor heterogeneity in glioblastoma: how far has multimodal imaging come?
Abstract
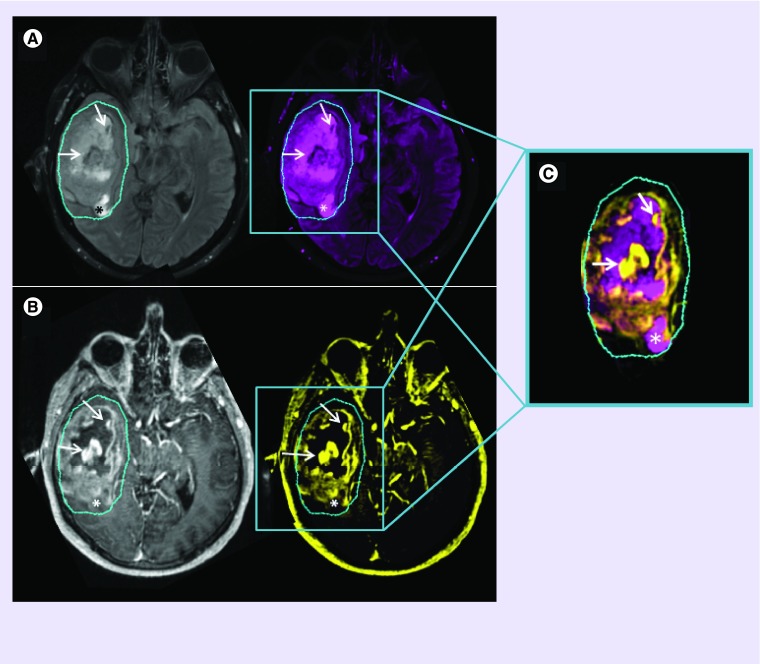
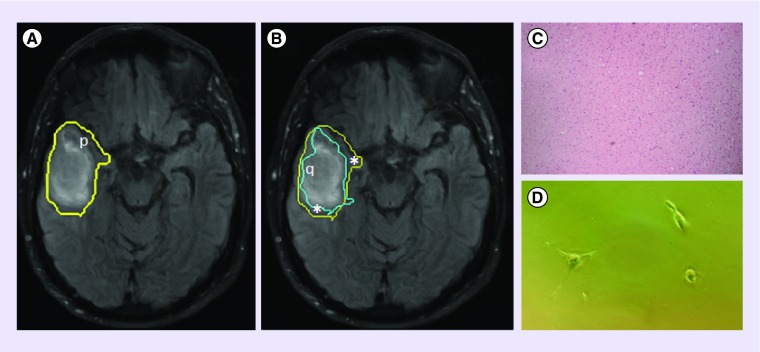
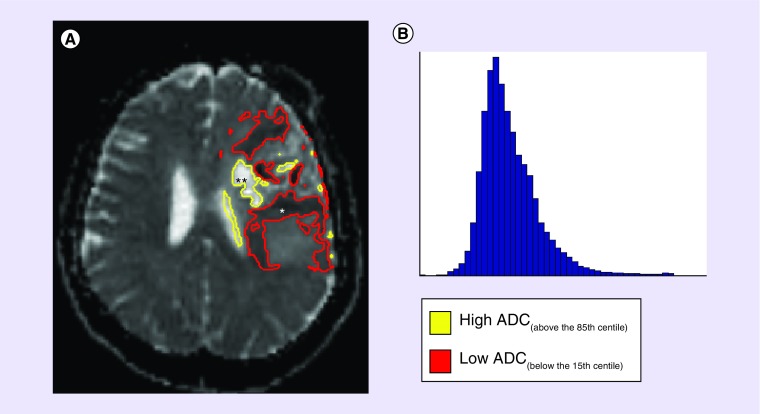
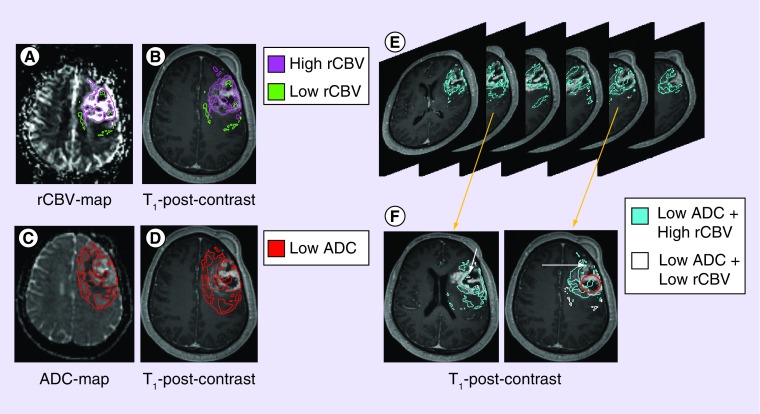
Glioblastoma demonstrates imaging features of intratumor heterogeneity that result from underlying heterogeneous biological properties. This stems from variations in cellular behavior that result from genetic mutations that either drive, or are driven by, heterogeneous microenvironment conditions. Among all imaging methods available, only T1-weighted contrast-enhancing and T2-weighted fluid-attenuated inversion recovery are used in standard clinical glioblastoma assessment and monitoring. Advanced imaging modalities are still considered emerging techniques as appropriate end points and robust methodologies are missing from clinical trials. Discovering how these images specifically relate to the underlying tumor biology may aid in improving quality of clinical trials and understanding the factors involved in regional responses to treatment, including variable drug uptake and effect of radiotherapy. Upon validation and standardization of emerging MR techniques, providing information based on the underlying tumor biology, these images may allow for clinical decision-making that is tailored to an individual's response to treatment.
Keywords: advanced imaging; glioblastoma; intratumor heterogeneity; subregional assessment; underlying biology.
Conflict of interest statement
Figures
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005;352(10):987–996. - PubMed
-
• The major single advancement in GBM treatment over the past years, incorporating RT with concomitant and adjuvant temozolomide.
-
- Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulen H-J. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre Phase III trial. Lancet Oncol. 2006;7(5):392–401. - PubMed
-
- Deacon J, Peckham MJ, Steel GG. The radioresponsiveness of human tumours and the initial slope of the cell survival curve. Radiother. Oncol. 1984;2(4):317–323. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical