

Organ Preservation in Rectal Adenocarcinoma: a phase II randomized controlled trial evaluating 3-year disease-free survival in patients with locally advanced rectal cancer treated with chemoradiation plus induction or consolidation chemotherapy, and total mesorectal excision or nonoperative management
- PMID: 26497495
- PMCID: PMC4619249
- DOI: 10.1186/s12885-015-1632-z
Organ Preservation in Rectal Adenocarcinoma: a phase II randomized controlled trial evaluating 3-year disease-free survival in patients with locally advanced rectal cancer treated with chemoradiation plus induction or consolidation chemotherapy, and total mesorectal excision or nonoperative management
Abstract
Background: Treatment of patients with non-metastatic, locally advanced rectal cancer (LARC) includes pre-operative chemoradiation, total mesorectal excision (TME) and post-operative adjuvant chemotherapy. This trimodality treatment provides local tumor control in most patients; but almost one-third ultimately die from distant metastasis. Most survivors experience significant impairment in quality of life (QoL), due primarily to removal of the rectum. A current challenge lies in identifying patients who could safely undergo rectal preservation without sacrificing survival benefit and QoL.
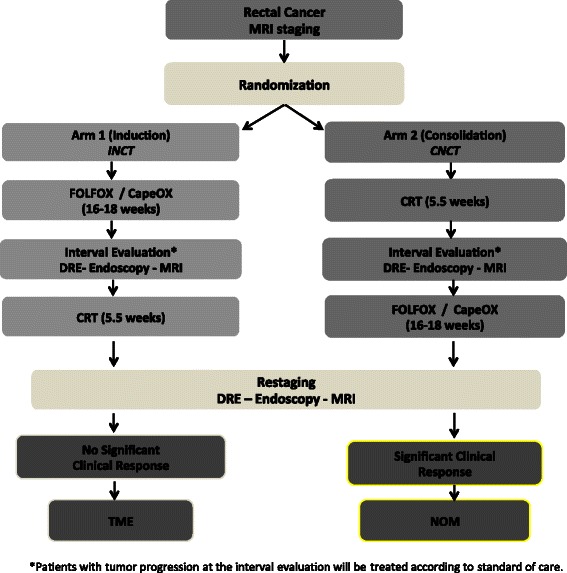
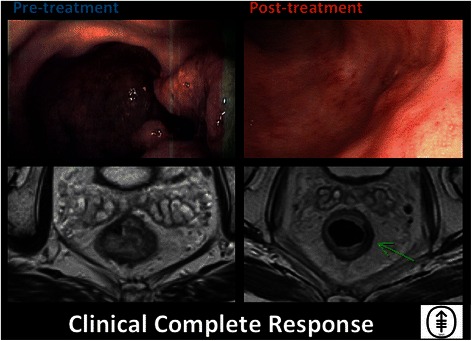
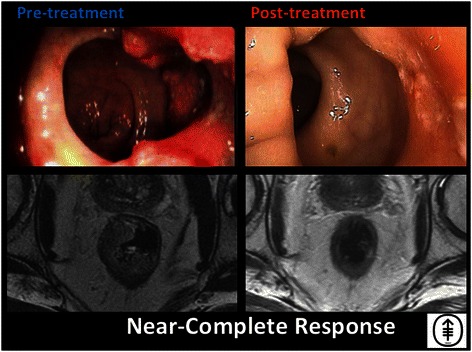
Methods/design: This multi-institutional, phase II study investigates the efficacy of total neoadjuvant therapy (TNT) and selective non-operative management (NOM) in LARC. Patients with MRI-staged Stage II or III rectal cancer amenable to TME will be randomized to receive FOLFOX/CAPEOX: a) before induction neoadjuvant chemotherapy (INCT); or b) after consolidation neoadjuvant chemotherapy (CNCT), with 5-FU or capecitabine-based chemoradiation. Patients in both arms will be re-staged after completing all neoadjuvant therapy. Those with residual tumor at the primary site will undergo TME. Patients with clinical complete response (cCR) will receive non-operative management (NOM). NOM patients will be followed every 3 months for 2 years, and every 6 months thereafter. TME patients will be followed according to NCCN guidelines. All will be followed for at least 5 years from the date of surgery or--in patients treated with NOM--the last day of treatment.
Discussion: The studies published thus far on the safety of NOM in LARC have compared survival between select groups of patients with a cCR after NOM, to patients with a pathologic complete response (pCR) after TME. The current study compares 3-year disease-free survival (DFS) in an entire population of patients with LARC, including those with cCR and those with pCR. We will compare the two arms of the study with respect to organ preservation at 3 years, treatment compliance, adverse events and surgical complications. We will measure QoL in both groups. We will analyze molecular indications that may lead to more individually tailored treatments in the future. This will be the first NOM trial utilizing a regression schema for response assessment in a prospective fashion.
Trial registration: NCT02008656.
Figures
References
-
- Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens J-H, Liersch T, Schmidberger H, Raab R. Preoperative versus postoperative chemoradiotherapy for rectal cancer. New Engl J Med. 2004;351:1731–1740. doi: 10.1056/NEJMoa040694. - DOI - PubMed
-
- Pucciarelli S, Del Bianco P, Efficace F, Serpentini S, Capirci C, De Paoli A, Amato A, Cuicchi D, Nitti D. Patient-reported outcomes after neoadjuvant chemoradiotherapy for rectal cancer: a multicenter prospective observational study. Ann Surg. 2011;253:71–77. doi: 10.1097/SLA.0b013e3181fcb856. - DOI - PubMed
-
- Bosset J-F, Calais G, Mineur L, Maingon P, Stojanovic-Rundic S, Bensadoun R-J, Bardet E, Beny A, Ollier J-C, Bolla M, Marchal D, Van Laethem J-L, Klein V, Giralt J, Clavère P, Glanzmann C, Cellier P, Collette L. Fluorouracil-based adjuvant chemotherapy after preoperative chemoradiotherapy in rectal cancer: long-term results of the EORTC 22921 randomised study. Lancet Oncol. 2014;15:184–190. doi: 10.1016/S1470-2045(13)70599-0. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
