

White matter abnormalities are associated with chronic postconcussion symptoms in blast-related mild traumatic brain injury
- PMID: 26497829
- PMCID: PMC4760357
- DOI: 10.1002/hbm.23022
White matter abnormalities are associated with chronic postconcussion symptoms in blast-related mild traumatic brain injury
Abstract
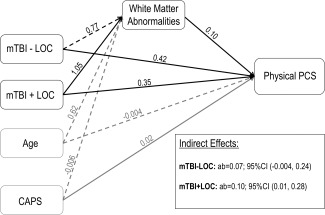
Blast-related mild traumatic brain injury (mTBI) is a common injury among Iraq and Afghanistan military veterans due to the frequent use of improvised explosive devices. A significant minority of individuals with mTBI report chronic postconcussion symptoms (PCS), which include physical, emotional, and cognitive complaints. However, chronic PCS are nonspecific and are also associated with mental health disorders such as posttraumatic stress disorder (PTSD). Identifying the mechanisms that contribute to chronic PCS is particularly challenging in blast-related mTBI, where the incidence of comorbid PTSD is high. In this study, we examined whether blast-related mTBI is associated with diffuse white matter changes, and whether these neural changes are associated with chronic PCS. Ninety Operation Enduring Freedom/Operation Iraqi Freedom (OEF/OIF) veterans were assigned to one of three groups including a blast-exposed no--TBI group, a blast-related mTBI without loss of consciousness (LOC) group (mTBI--LOC), and a blast-related mTBI with LOC group (mTBI + LOC). PCS were measured with the Rivermead Postconcussion Questionnaire. Results showed that participants in the mTBI + LOC group had more spatially heterogeneous white matter abnormalities than those in the no--TBI group. These white matter abnormalities were significantly associated with physical PCS severity even after accounting for PTSD symptoms, but not with cognitive or emotional PCS severity. A mediation analysis revealed that mTBI + LOC significantly influenced physical PCS severity through its effect on white matter integrity. These results suggest that white matter abnormalities are associated with chronic PCS independent of PTSD symptom severity and that these abnormalities are an important mechanism explaining the relationship between mTBI and chronic physical PCS.
Keywords: OEF/OIF; PTSD; diffusion tensor imaging; loss of consciousness.
Published 2015. This article is a U.S. Government work and is in the public domain in the USA.
Figures



References
-
- American Congress of Rehabilitation Medicine (1993): Definition of mild traumatic brain injury. J Head Trauma Rehabil 8:86–87.
-
- Bartnik‐Olson BL, Holshouser B, Wang H, Grube M, Tong K, Wong V, Ashwal S (2014): Impaired neurovascular unit function contributes to persistent symptoms after concussion: A pilot study. J Neurotrauma 31:1497–1506. - PubMed
-
- Bazarian JJ, Donnelly K, Peterson DR, Warner GC, Zhu T, Zhong J (2012): The relation between posttraumatic stress disorder and mild traumatic brain injury acquired during operations enduring freedom and iraqi freedom. J Head Trauma Rehabil 28:1–12. - PubMed
-
- Bazarian JJ, Zhong J, Blyth B, Zhu T, Kavcic V, Peterson D (2007): Diffusion tensor imaging detects clinically important axonal damage after mild traumatic brain injury: A pilot study. J Neurotrauma 24:1447–1459. - PubMed
-
- Belanger HG, Kretzmer T, Vanderploeg RD, French LM (2010): Symptom complaints following combat‐related traumatic brain injury: Relationship to traumatic brain injury severity and posttraumatic stress disorder. J Int Neuropsychol Soc 16:194–199. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
