

Patterns of resource utilization and cost for postmenopausal women with hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer in Europe
- PMID: 26498283
- PMCID: PMC4619560
- DOI: 10.1186/s12885-015-1762-3
Patterns of resource utilization and cost for postmenopausal women with hormone-receptor-positive, human epidermal growth factor receptor-2-negative advanced breast cancer in Europe
Abstract
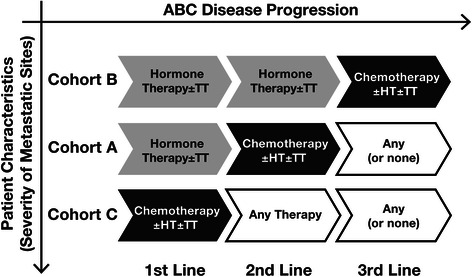
Background: Healthcare resource utilization in breast cancer varies by disease characteristics and treatment choices. However, lack of clarity in guidelines can result in varied interpretation and heterogeneous treatment management and costs. In Europe, the extent of this variability is unclear. Therefore, evaluation of chemotherapy use and costs versus hormone therapy across Europe is needed.
Methods: This retrospective chart review (N = 355) examined primarily direct costs for chemotherapy versus hormone therapy in postmenopausal women with hormone-receptor-positive (HR+), human epidermal growth factor receptor-2-negative (HER2-) advanced breast cancer across 5 European countries (France, Germany, The Netherlands, Belgium, and Sweden).
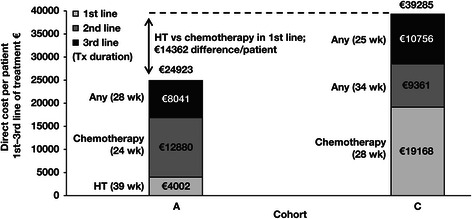
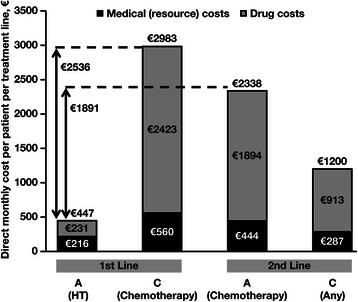
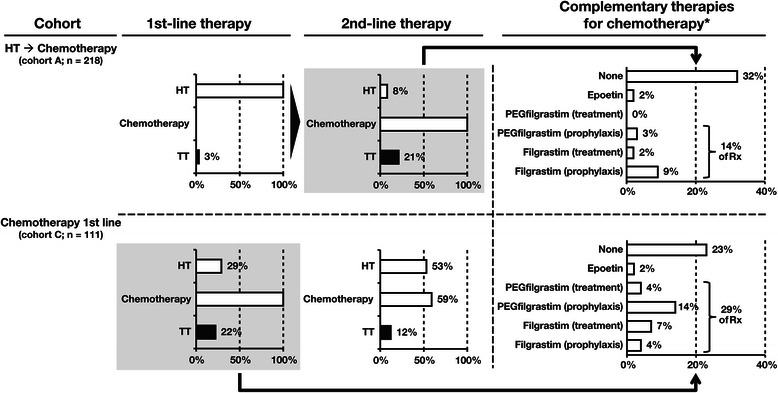
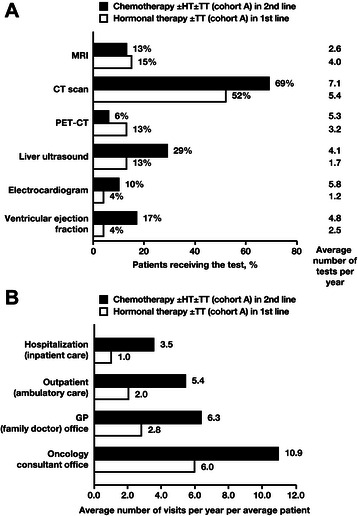
Results: Total direct costs across the first 3 treatment lines were approximately €10,000 to €14,000 lower for an additional line of hormone therapy-based treatment versus switching to chemotherapy-based treatment. Direct cost difference between chemotherapy-based and hormone therapy-based regimens was approximately €1900 to €2500 per month. Chemotherapy-based regimens were associated with increased resource utilization (managing side effects; concomitant targeted therapy use; and increased frequencies of hospitalizations, provider visits, and monitoring tests). The proportion of patients taking sick leave doubled after switching from hormone therapy to chemotherapy.
Conclusions: These results suggest chemotherapy is associated with increased direct costs and potentially with increased indirect costs (lower productivity of working patients) versus hormone therapy in HR+, HER2- advanced breast cancer.
Figures
References
-
- International Agency for Research on Cancer, European Cancer Observatory. EUCAN factsheets: Breast cancer, 2012. http://eco.iarc.fr/EUCAN/CancerOne.aspx?Cancer=46&Gender=2. (2012). Accessed 26 Mar 2014.
-
- Luengo-Fernandez R, Leal J, Sullivan R. Economic burden of malignant neoplasms in the European Union. Vienna: Presented at: ESMO 2012 Congress; 2012.
-
- European Society for Medical Oncology. ESMO 2012 press release: the true costs of cancer in Europe revealed. http://www.esmo.org/Conferences/Past-Conferences/ESMO-2012-Congress/News.... (2012). Accessed 26 Mar 2014.
-
- Arbeitsgemeinschaft Gynakologische Onkologie E.V. (AGO). AGO Breast Committee: Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer. Recommendations 2014. http://www.ago-online.de. (2014). Accessed 16 Sep 2014.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
