

Estimation of changes in the force of infection for intestinal and urogenital schistosomiasis in countries with schistosomiasis control initiative-assisted programmes
- PMID: 26499981
- PMCID: PMC4619997
- DOI: 10.1186/s13071-015-1138-1
Estimation of changes in the force of infection for intestinal and urogenital schistosomiasis in countries with schistosomiasis control initiative-assisted programmes
Abstract
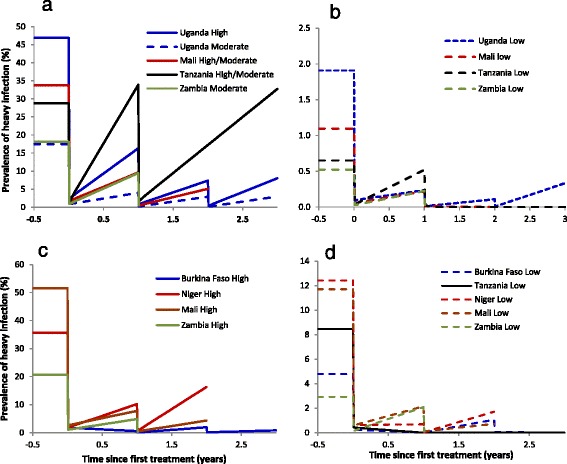
Background: The last decade has seen an expansion of national schistosomiasis control programmes in Africa based on large-scale preventative chemotherapy. In many areas this has resulted in considerable reductions in infection and morbidity levels in treated individuals. In this paper, we quantify changes in the force of infection (FOI), defined here as the per (human) host parasite establishment rate, to ascertain the impact on transmission of some of these programmes under the umbrella of the Schistosomiasis Control Initiative (SCI).
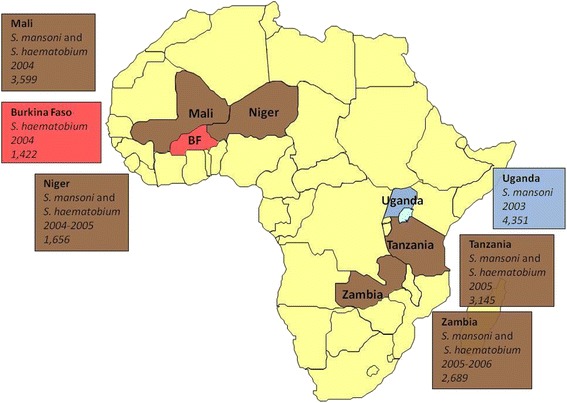
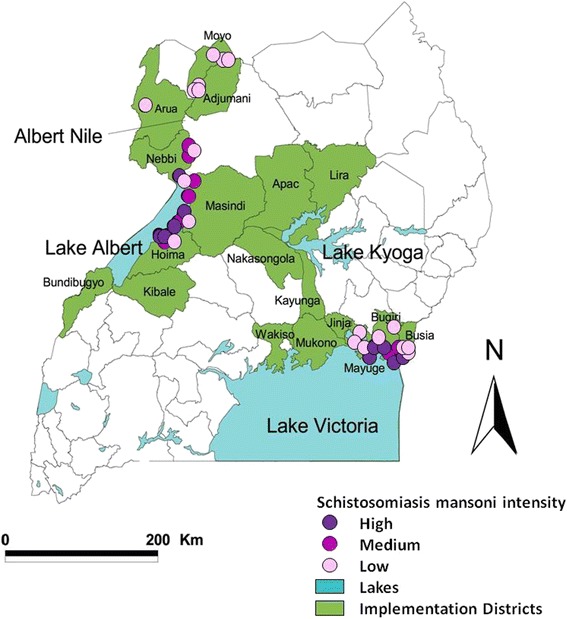
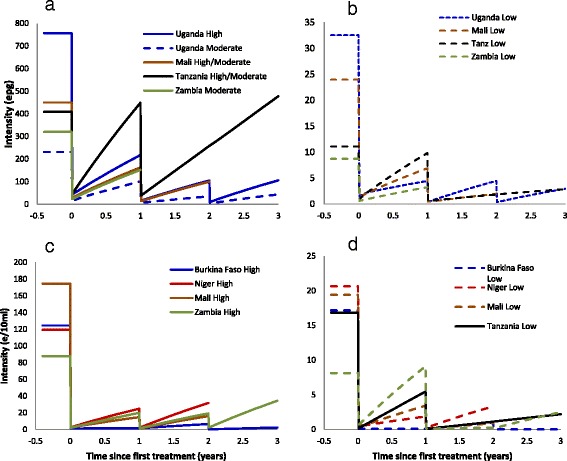
Methods: A previous model for the transmission dynamics of Schistosoma mansoni was adapted here to S. haematobium. These models were fitted to longitudinal cohort (infection intensity) monitoring and evaluation data. Changes in the FOI following up to three annual rounds of praziquantel were estimated for Burkina Faso, Mali, Niger, Tanzania, Uganda, and Zambia in sub-Saharan Africa (SSA) according to country, baseline endemicity and schistosome species. Since schistosomiasis transmission is known to be highly focal, changes in the FOI at a finer geographical scale (that of sentinel site) were also estimated for S. mansoni in Uganda.
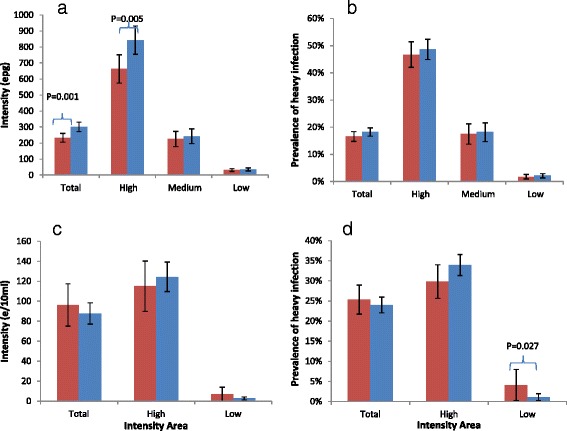
Results: Substantial and statistically significant reductions in the FOI relative to baseline were recorded in the majority of, but not all, combinations of country, parasite species, and endemicity areas. At the finer geographical scale assessed within Uganda, marked heterogeneity in the magnitude and direction of the relative changes in FOI was observed that would not have been appreciated by a coarser-scale analysis.
Conclusions: Reductions in the rate at which humans acquire schistosomes have been achieved in many areas of SSA countries assisted by the SCI, while challenges in effectively reducing transmission persist in others. Understanding the underlying heterogeneity in the impact and performance of the control intervention at the level of the transmission site will become increasingly important for programmes transitioning from morbidity reduction to elimination of infection. Such analyses will require a fine-scale approach. The lack of association found between programmatic variables, such as therapeutic treatment coverage (recorded at district level) and changes in FOI (at sentinel site level) is discussed and recommendations are made.
Figures
References
-
- Fenwick A, Webster JP, Bosqué-Oliva E, Blair L, Fleming FM, Zhang Y, et al. The Schistosomiasis Control Initiative (SCI): rationale, development and implementation from 2002–2008. Parasitology. 2009;136:1719–30. - PubMed
-
- Anderson RM, May RM. Infectious Diseases of Humans: Dynamics and Control. Oxford: Oxford University Press; 1991.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
