

Biodegradable collagen matrix (Ologen™) implant and conjunctival autograft for scleral necrosis after pterygium excision: two case reports
- PMID: 26499993
- PMCID: PMC4619331
- DOI: 10.1186/s12886-015-0130-z
Biodegradable collagen matrix (Ologen™) implant and conjunctival autograft for scleral necrosis after pterygium excision: two case reports
Abstract
Background: Scleromalacia, in the form of scleral thinning, melting, and necrosis, is a potentially serious complication of pterygium excision. This study introduces a new biodegradable material, Ologen™ collagen matrix (OCM), to repair scleral thinning as an alternative to preserved scleral tissue, and evaluates the long-term outcomes of OCM for ocular surface reconstruction surgery.
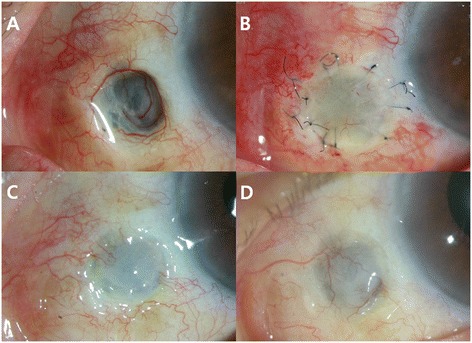
Case presentation: Two cases of possibly mitomycin C (MMC)-associated marked scleral thinning after pterygium excision with 0.02 % topical MMC for 2-weeks were included in this study. An OCM graft at the scleral thinning area and conjunctival autograft (CAU) were performed on both patients. The scleral defect size was measured and its margin was marked with a biopsy punch. The margin of the scleral thinning area was trimmed by Vannas scissors and the OCM was cut using a circular-shape biopsy punch of the same size. The OCM was sutured with a recipient scleral wall using 10-0 nylon interrupted sutures. Free CAU was harvested from the superonasal bulbar conjunctiva with a punch biopsy 1-mm larger in diameter than that of the OCM. The previously sutured OCM bed was covered with CAU and the graft was secured with 10-0 nylon interrupted sutures. Both patients were examined periodically for over two years by assessing graft thickness and surface vascularization using a slit lamp biomicroscope. Reepithelialization of the ocular surface was observed within three to six days after surgery. Ocular discomfort and inflammation ceased in both patients as the ocular surface quickly stabilized. The entire graft site remained intact and provided a good healthy ocular surface with fluorescein stain negative intact epithelium and good vascularization of grafted conjunctiva. Epithelial defects and scleral thinning did not recur in either patient over the two year follow-up period.
Conclusion: For treatment of a possibly MMC-associated scleral necrosis following the surgical excision of the pterygium, an OCM graft with CAU is highly recommended for good clinical outcomes and low recurrence rates. With the clinical results of this study, the new biodegradable Ologen™ collagen matrix qualifies as an alternative treatment to scleral tissue for ocular surface reconstruction.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
