

Association between Serum Potassium and Outcomes in Patients with Reduced Kidney Function
- PMID: 26500246
- PMCID: PMC4702219
- DOI: 10.2215/CJN.01730215
Association between Serum Potassium and Outcomes in Patients with Reduced Kidney Function
Abstract
Background and objectives: Patients with CKD are more likely than others to have abnormalities in serum potassium (K(+)). Aside from severe hyperkalemia, the clinical significance of K(+) abnormalities is not known. We sought to examine the association of serum K(+) with mortality and hospitalization rates within narrow eGFR strata to understand how the burden of hyperkalemia varies by CKD severity. Associations were examined between serum K(+) and discontinuation of medications that block the renin-angiotensin-aldosterone system (RAAS), which are known to increase serum K(+).
Design, setting, participants, & measurements: A cohort of patients with CKD (eGFR<60 ml/min per 1.73 m(2)) with serum K(+) data were studied (n=55,266) between January 1, 2009, and June 30, 2013 (study end). Serum K(+), eGFR, and covariates were considered on a time-updated basis. Mortality, major adverse cardiovascular events (MACE), hospitalization, and discontinuation of RAAS blockers were considered per time at risk.
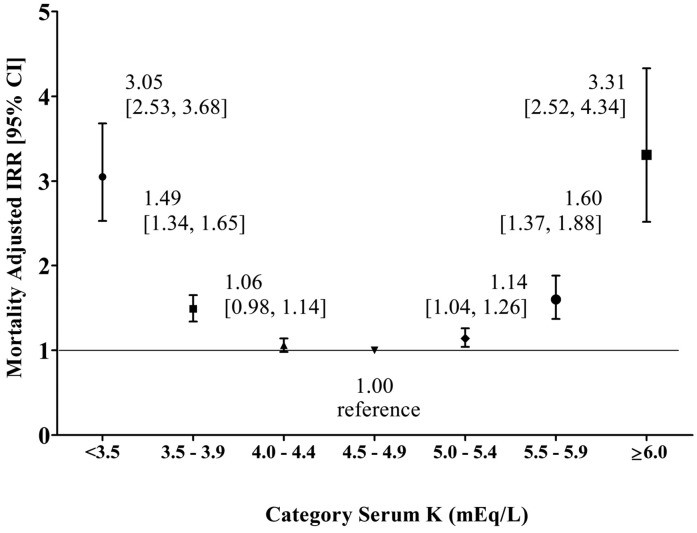
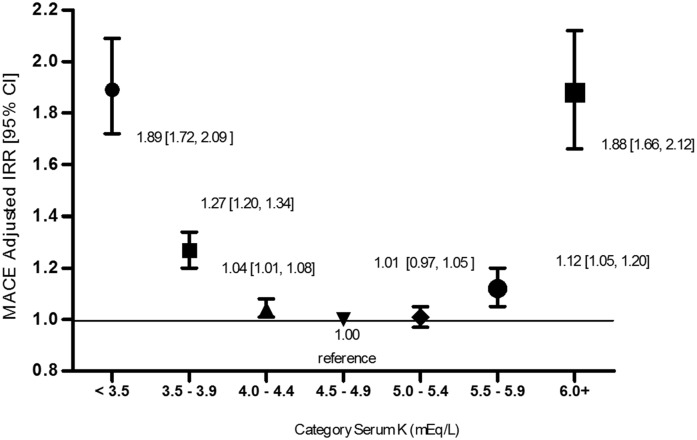
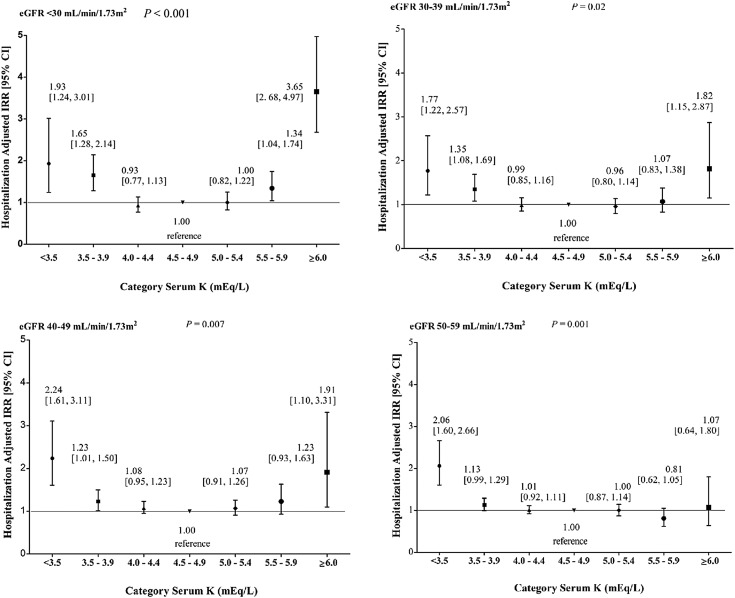
Results: During the study, serum K(+) levels of 5.5-5.9 and ≥6.0 mEq/L were most prevalent at lower eGFR: they were present, respectively, in 1.7% and 0.2% of patient-time for eGFR of 50-59 ml/min per 1.73 m(2) versus 7.6% and 1.8% of patient-time for eGFR<30 ml/min per 1.73 m(2). Serum K(+) level <3.5 mEq/L was present in 1.2%-1.4% of patient-time across eGFR strata. The median follow-up time was 2.76 years. There was a U-shaped association between serum K(+) and mortality; pooled adjusted incidence rate ratios were 3.05 (95% confidence interval, 2.53 to 3.68) and 3.31 (95% confidence interval, 2.52 to 4.34) for K(+) levels <3.5 mEq/L and ≥6.0 mEq/L, respectively. Within eGFR strata, there were U-shaped associations of serum K(+) with rates of MACE, hospitalization, and discontinuation of RAAS blockers.
Conclusions: Both hyperkalemia and hypokalemia were independently associated with higher rates of death, MACE, hospitalization, and discontinuation of RAAS blockers in patients with CKD who were not undergoing dialysis. Future studies are needed to determine whether interventions targeted at maintaining normal serum K(+) improve outcomes in this population.
Keywords: ACE inhibitors; chronic kidney disease; follow-up studies; glomerular filtration rate; hospitalization; humans; hyperkalemia; hypokalemia; mortality; potassium.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
