

WSES position paper on vascular emergency surgery
- PMID: 26500690
- PMCID: PMC4618918
- DOI: 10.1186/s13017-015-0037-2
WSES position paper on vascular emergency surgery
Abstract
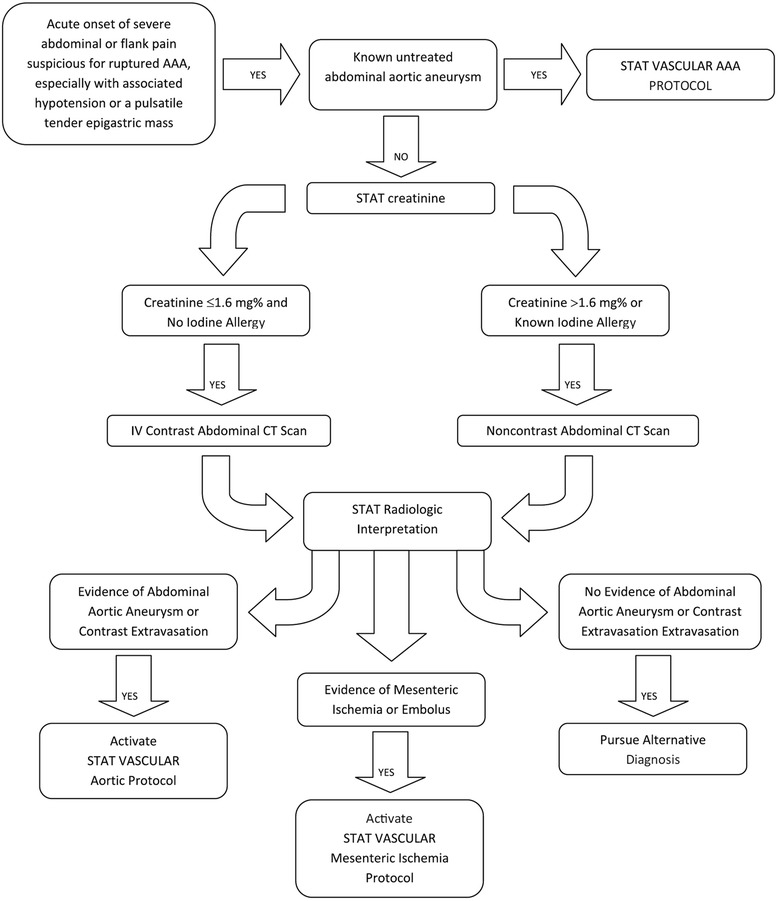
Trauma, both blunt and penetrating, is extremely common worldwide, as trauma to major vessels. The management of these patients requires specialized surgical skills and techniques of the trauma surgeon. Furthermore few other surgical emergencies require immediate diagnosis and treatment like a ruptured abdominal aortic aneurysm (rAAA). Mortality of patients with a rAAA reaches 85 %, with more than half dying before reaching the hospital. These are acute events demanding immediate intervention to save life and limb and precluding any attempt at transfer or referral. It is the purpose of this position paper to discuss neck, chest, extremities and abdominal trauma, bringing to light recent evidence based data as well as expert opinions; besides, in this paper we present a review of the recent literature on rAAA and we discuss the rationale for transfer to referral center, the role of preoperative imaging and the pros and cons of Endoluminal repair of rAAA (REVAR) versus Open Repair (OR).
Keywords: Ruptured abdominal aorta aneurism; Trauma; Vascular Trauma: Neck, Chest and Extremities; Vascular control; Vascular injuries.
Figures


References
-
- Lakhwani MN, Gooi BH, Barras CD. Vascular trauma in Penang and Kuala Lumpur Hospitals. Med J Malays. 2002;57(4):426–32. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
