

Prevention of Primary Cytomegalovirus Infection in Pregnancy
- PMID: 26501119
- PMCID: PMC4588434
- DOI: 10.1016/j.ebiom.2015.08.003
Prevention of Primary Cytomegalovirus Infection in Pregnancy
Abstract
Background: Cytomegalovirus (CMV) is the leading infectious agent causing congenital sensorineural hearing loss and psychomotor retardation. CMV vaccine is currently unavailable and treatment options in pregnancy are limited. Susceptible pregnant women caring for children are at high risk for primary infection. CMV educational and hygienic measures have the potential to prevent primary maternal infection.
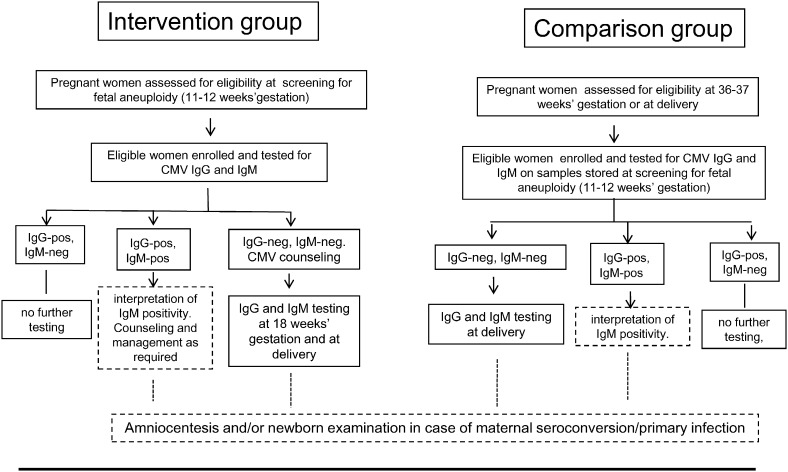
Methods: A mixed interventional and observational controlled study was conducted to investigate the effectiveness of hygiene information among pregnant women at risk for primary CMV infection for personal/occupational reasons. In the intervention arm, CMV-seronegative women, identified at the time of maternal serum screening for fetal aneuploidy at 11-12 weeks of gestation, were given hygiene information and prospectively tested for CMV until delivery. The comparison arm consisted of women enrolled at delivery who were neither tested for nor informed about CMV during pregnancy, and who had a serum sample stored at the screening for fetal aneuploidy. By design, groups were homogeneous for age, parity, education, and exposure to at least one risk factor. The primary outcome was CMV seroconversion. Acceptance of hygiene recommendations was a secondary objective and was measured by a self-report.
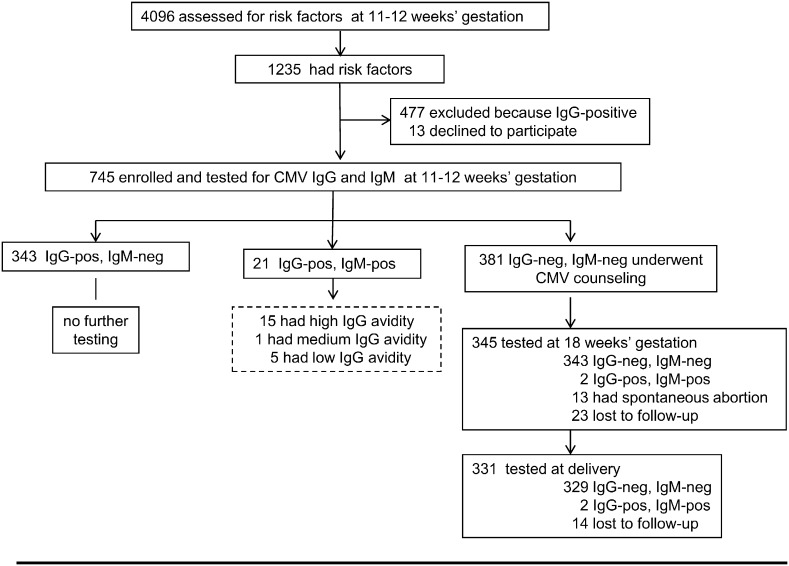
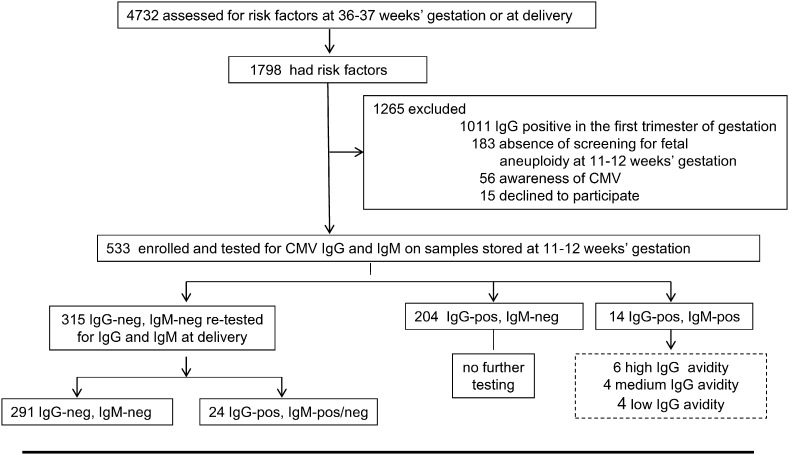
Findings: Four out of 331 (1.2%) women seroconverted in the intervention group compared to 24/315 (7.6%) in the comparison group (delta = 6.4%; 95% CI 3.2-9.6; P < 0.001). There were 3 newborns with congenital infection in the intervention group and 8 in the comparison group (1 with cerebral ultrasound abnormalities at birth). Ninety-three percent of women felt hygiene recommendations were worth suggesting to all pregnant women at risk for infection.
Interpretation: This controlled study provides evidence that an intervention based on the identification and hygiene counseling of CMV-seronegative pregnant women significantly prevents maternal infection. While waiting for CMV vaccine to become available, the intervention described may represent a responsible and acceptable primary prevention strategy to reduce congenital CMV.
Keywords: Cytomegalovirus; Hygiene measures; Pregnancy; Prevention; Primary infection.
Figures
References
-
- Adler S.P. Molecular epidemiology of cytomegalovirus: evidence for viral transmission to parents from children infected at a day care center. Pediatr. Infect. Dis. 1986;5:315–318. - PubMed
-
- Adler S.P., Finney J.W., Manganello A.M., Best A.M. Prevention of child-to-mother transmission of cytomegalovirus by changing behaviours: a randomized controlled trial. Pediatr. Infect. Dis. J. 1996;15:240–246. - PubMed
-
- Adler S.P., Finney J.W., Manganello A.M., Best A.M. Prevention of child-to-mother transmission of cytomegalovirus among pregnant women. J. Pediatr. 2004;145:485–491. - PubMed
-
- Arvin A.M., Fast P., Myers M., Plotkin S., Rabinovich R. Vaccine development to prevent cytomegalovirus disease: report from the national vaccine advisory committee. Clin. Infect. Dis. 2004;39:233–239. - PubMed
-
- Breugelmans M., Naessens A., Foulon W. Prevention of toxoplasmosis during pregnancy — an epidemiological survey over 22 consecutive years. J. Perinat. Med. 2004;32:211–214. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
