

Evaluation of Perioperative Medication Errors and Adverse Drug Events
- PMID: 26501385
- PMCID: PMC4681677
- DOI: 10.1097/ALN.0000000000000904
Evaluation of Perioperative Medication Errors and Adverse Drug Events
Abstract
Background: The purpose of this study is to assess the rates of perioperative medication errors (MEs) and adverse drug events (ADEs) as percentages of medication administrations, to evaluate their root causes, and to formulate targeted solutions to prevent them.
Methods: In this prospective observational study, anesthesia-trained study staff (anesthesiologists/nurse anesthetists) observed randomly selected operations at a 1,046-bed tertiary care academic medical center to identify MEs and ADEs over 8 months. Retrospective chart abstraction was performed to flag events that were missed by observation. All events subsequently underwent review by two independent reviewers. Primary outcomes were the incidence of MEs and ADEs.
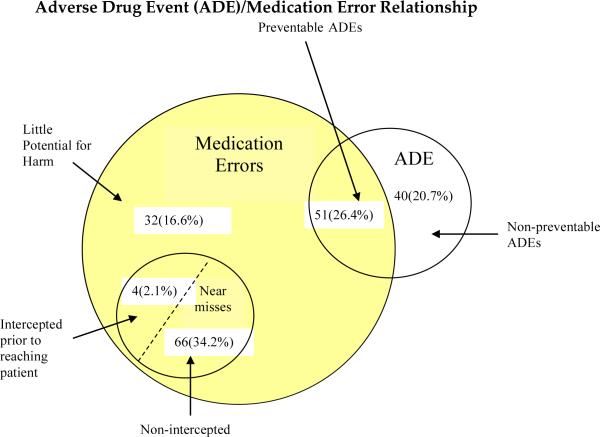
Results: A total of 277 operations were observed with 3,671 medication administrations of which 193 (5.3%; 95% CI, 4.5 to 6.0) involved a ME and/or ADE. Of these, 153 (79.3%) were preventable and 40 (20.7%) were nonpreventable. The events included 153 (79.3%) errors and 91 (47.2%) ADEs. Although 32 (20.9%) of the errors had little potential for harm, 51 (33.3%) led to an observed ADE and an additional 70 (45.8%) had the potential for patient harm. Of the 153 errors, 99 (64.7%) were serious, 51 (33.3%) were significant, and 3 (2.0%) were life-threatening.
Conclusions: One in 20 perioperative medication administrations included an ME and/or ADE. More than one third of the MEs led to observed ADEs, and the remaining two thirds had the potential for harm. These rates are markedly higher than those reported by retrospective surveys. Specific solutions exist that have the potential to decrease the incidence of perioperative MEs.
Figures
Comment in
-
Perioperative Medication Errors: Building Safer Systems.Anesthesiology. 2016 Jan;124(1):1-3. doi: 10.1097/ALN.0000000000000905. Anesthesiology. 2016. PMID: 26501388 No abstract available.
-
Evaluation of Perioperative Medication Errors.Anesthesiology. 2016 Aug;125(2):429-31. doi: 10.1097/ALN.0000000000001185. Anesthesiology. 2016. PMID: 27433762 No abstract available.
-
Adverse Drug Events Link to Severity of the Event Data Needed.Anesthesiology. 2016 Aug;125(2):431. doi: 10.1097/ALN.0000000000001186. Anesthesiology. 2016. PMID: 27433763 No abstract available.
-
Counting Errors: Medication or Medical?Anesthesiology. 2016 Aug;125(2):431-2. doi: 10.1097/ALN.0000000000001187. Anesthesiology. 2016. PMID: 27433764 No abstract available.
-
In Reply.Anesthesiology. 2016 Aug;125(2):432-7. doi: 10.1097/ALN.0000000000001188. Anesthesiology. 2016. PMID: 27433765 Free PMC article. No abstract available.
-
A new paradigm for medication error research.Br J Anaesth. 2019 Oct;123(4):e483-e484. doi: 10.1016/j.bja.2019.06.015. Epub 2019 Jul 19. Br J Anaesth. 2019. PMID: 31331648 No abstract available.
-
The importance of pharmacists in modern day surgery - editorial.Int J Surg. 2023 Feb 1;109(2):88-90. doi: 10.1097/JS9.0000000000000146. Int J Surg. 2023. PMID: 36799812 Free PMC article. No abstract available.
References
-
- Merry AF, Webster CS, Hannam J, Mitchell SJ, Henderson R, Reid P, Edwards KE, Jardim A, Pak N, Cooper J, Hopley L, Frampton C, Short TG. Multimodal system designed to reduce errors in recording and administration of drugs in anaesthesia: prospective randomised clinical evaluation. BMJ. 2011;343:d5543. - PMC - PubMed
-
- Fasting S, Gisvold SE. Adverse drug errors in anesthesia, and the impact of coloured syringe labels. Can J Anaesth. 2000;47(11):1060–7. - PubMed
-
- Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology. 1984;60(1):34–42. - PubMed
-
- Webster CS, Merry AF, Larsson L, McGrath KA, Weller J. The frequency and nature of drug administration error during anaesthesia. Anaesth Intensive Care. 2001;29(5):494–500. - PubMed
-
- Orser BA, Chen RJ, Yee DA. Medication errors in anesthetic practice: a survey of 687 practitioners. Can J Anaesth. 2001;48(2):139–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
