

Pulmonary Artery Enlargement Is Associated With Cardiac Injury During Severe Exacerbations of COPD
- PMID: 26501747
- PMCID: PMC4944777
- DOI: 10.1378/chest.15-1504
Pulmonary Artery Enlargement Is Associated With Cardiac Injury During Severe Exacerbations of COPD
Abstract
Background: Relative pulmonary arterial enlargement, defined by a pulmonary artery to aorta (PA/A) ratio > 1 on CT scanning, predicts hospitalization for acute exacerbations of COPD (AECOPD). However, it is unclear how AECOPD affect the PA/A ratio. We hypothesized that the PA/A ratio would increase at the time of AECOPD and that a ratio > 1 would be associated with worse clinical outcomes.
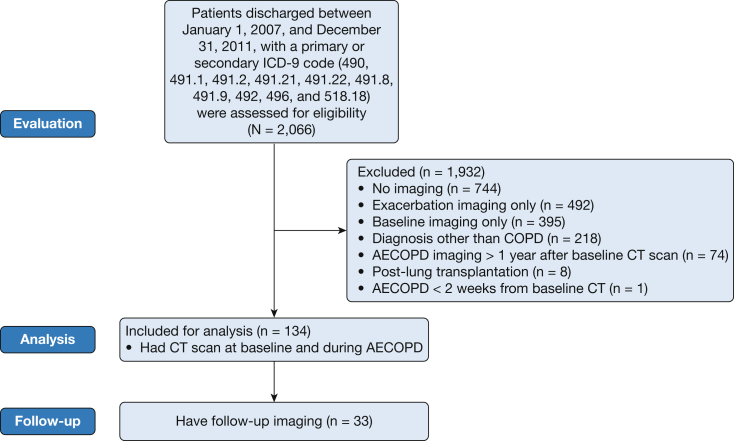
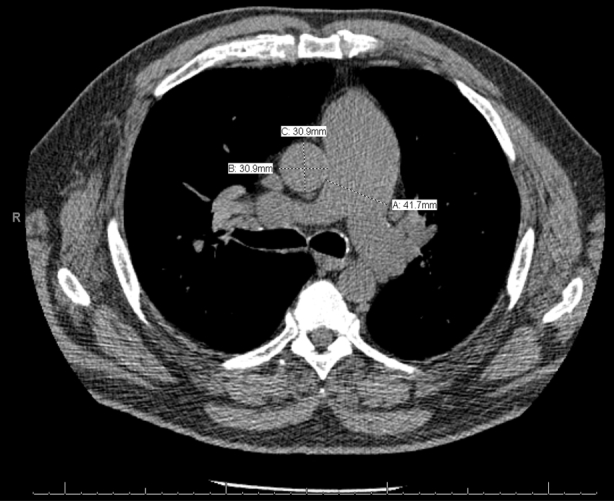
Methods: Patients discharged with an International Classification of Diseases, Ninth Revision, diagnosis of AECOPD from a single center over a 5-year period were identified. Patients were included who had a CT scan performed during the stable period prior to the index AECOPD episode as well as a CT scan at the time of hospitalization. A subset of patients also underwent postexacerbation CT scans. The pulmonary arterial diameter, ascending aortic diameter, and the PA/A ratio were measured on CT scans. Demographic data, comorbidities, troponin level, and hospital outcome data were analyzed.
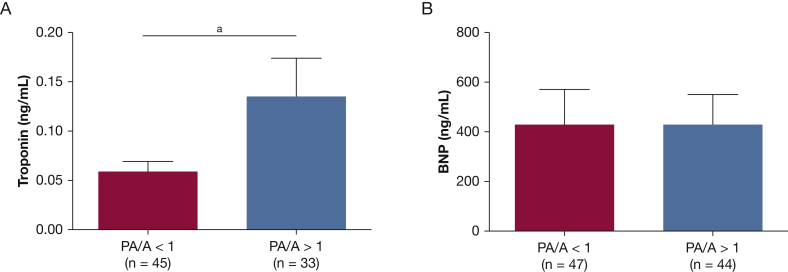
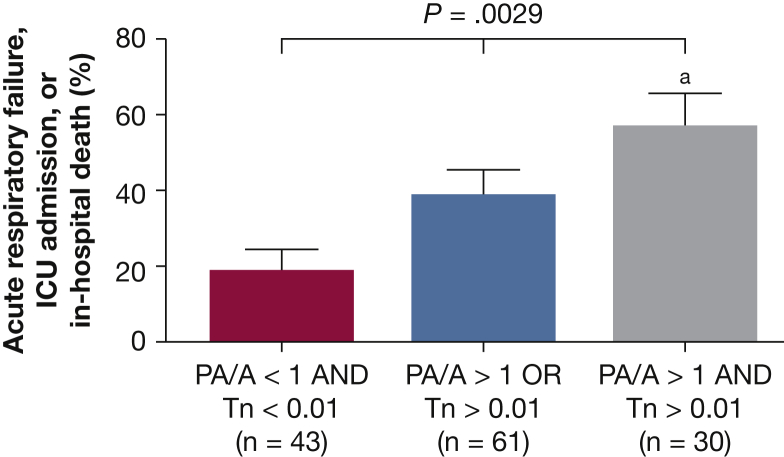
Results: A total of 134 patients were included in the study. They had a mean age of 65 ± 10 years, 47% were male, and 69% were white; overall, patients had a mean FEV1 of 47% ± 19%. The PA/A ratio increased from baseline at the time of exacerbation (0.97 ± 0.15 from 0.91 ± 0.17; P < .001). Younger age and known pulmonary hypertension were independently associated with an exacerbation PA/A ratio > 1. Patients with PA/A ratio > 1 had higher troponin values. Those with a PA/A ratio > 1 and troponin levels > 0.01 ng/mL had increased acute respiratory failure, ICU admission, or inpatient mortality compared with those without both factors (P = .0028). The PA/A ratio returned to baseline values following AECOPD.
Conclusions: The PA/A ratio increased at the time of severe AECOPD and a ratio > 1 predicted cardiac injury and a more severe hospital course.
Keywords: COPD; CT scan; acute exacerbation of COPD; enzymes (cardiology); pulmonary circulation.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
New Horizons in Obstructive Lung Disease. Microbiome Dynamics, Pulmonary Artery Enlargement, and Endobronchial Valves.Am J Respir Crit Care Med. 2017 Mar 15;195(6):824-826. doi: 10.1164/rccm.201609-1823RR. Am J Respir Crit Care Med. 2017. PMID: 28040986 No abstract available.
References
-
- Vestbo J., Hurd S.S., Agusti A.G. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. - PubMed
-
- Perera P.N., Armstrong E.P., Sherrill D.L., Skrepnek G.H. Acute exacerbations of COPD in the United States: inpatient burden and predictors of costs and mortality. COPD. 2012;9(2):131–141. - PubMed
-
- Khakban A., Sin D.D., FitzGerald J.M. Ten-year trends in direct costs of COPD: a population-based study. Chest. 2015;148(3):640–646. - PubMed
-
- McGhan R., Radcliff T., Fish R., Sutherland E.R., Welsh C., Make B. Predictors of rehospitalization and death after a severe exacerbation of COPD. Chest. 2007;132(6):1748–1755. - PubMed
-
- Anzueto A., Sethi S., Martinez F.J. Exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2007;4(7):554–564. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
