

Pharmacokinetics of Isoniazid, Pyrazinamide, and Ethambutol in Newly Diagnosed Pulmonary TB Patients in Tanzania
- PMID: 26501782
- PMCID: PMC4621059
- DOI: 10.1371/journal.pone.0141002
Pharmacokinetics of Isoniazid, Pyrazinamide, and Ethambutol in Newly Diagnosed Pulmonary TB Patients in Tanzania
Abstract
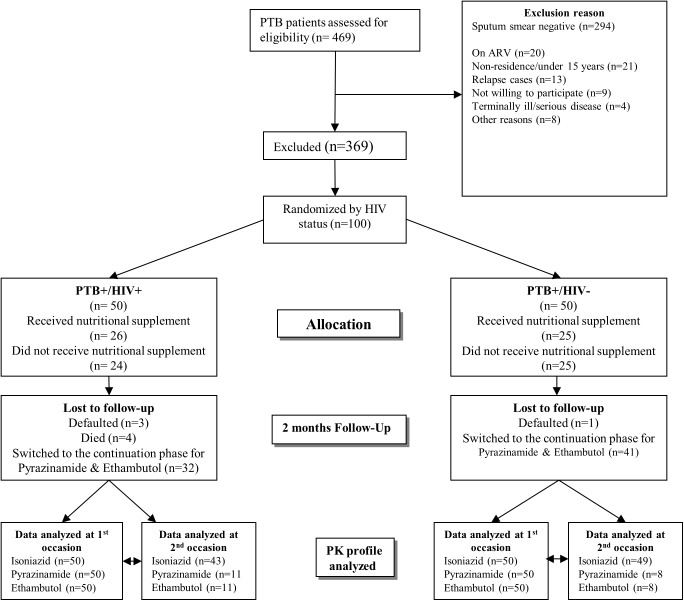
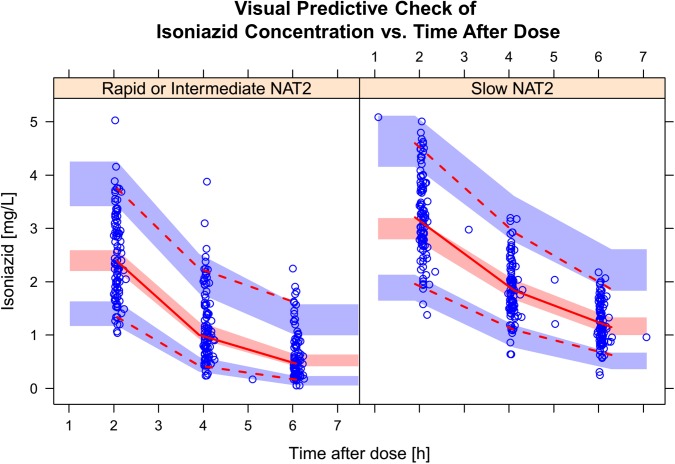
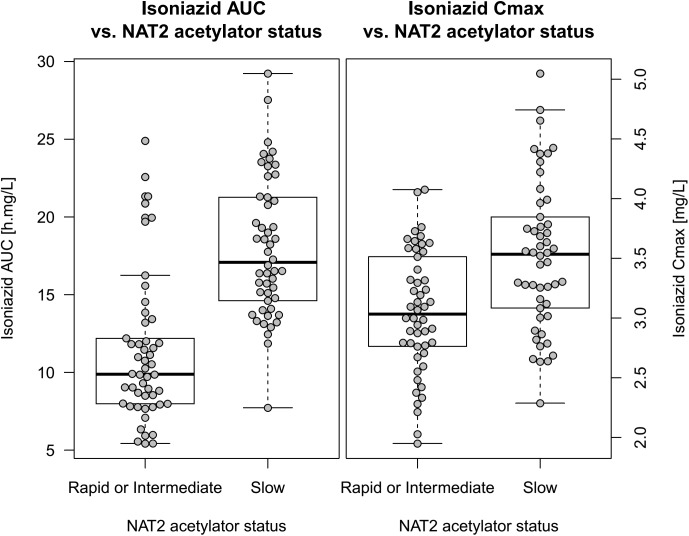
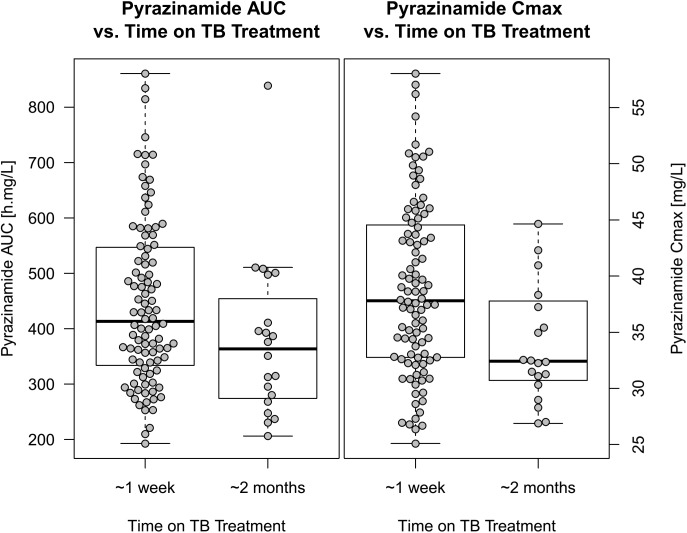
Exposure to lower-than-therapeutic levels of anti-tuberculosis drugs is likely to cause selection of resistant strains of Mycobacterium tuberculosis and treatment failure. The first-line anti-tuberculosis (TB) regimen consists of rifampicin, isoniazid, pyrazinamide, and ethambutol, and correct management reduces risk of TB relapse and development of drug resistance. In this study we aimed to investigate the effect of standard of care plus nutritional supplementation versus standard care on the pharmacokinetics of isoniazid, pyrazinamide and ethambutol among sputum smear positive TB patients with and without HIV. In a clinical trial in 100 Tanzanian TB patients, with or without HIV infection, drug concentrations were determined at 1 week and 2 months post initiation of anti-TB medication. Data was analysed using population pharmacokinetic modelling. The effect of body size was described using allometric scaling, and the effects of nutritional supplementation, HIV, age, sex, CD4+ count, weight-adjusted dose, NAT2 genotype, and time on TB treatment were investigated. The kinetics of all drugs was well characterised using first-order elimination and transit compartment absorption, with isoniazid and ethambutol described by two-compartment disposition models, and pyrazinamide by a one-compartment model. Patients with a slow NAT2 genotype had higher isoniazid exposure and a lower estimate of oral clearance (15.5 L/h) than rapid/intermediate NAT2 genotype (26.1 L/h). Pyrazinamide clearance had an estimated typical value of 3.32 L/h, and it was found to increase with time on treatment, with a 16.3% increase after the first 2 months of anti-TB treatment. The typical clearance of ethambutol was estimated to be 40.7 L/h, and was found to decrease with age, at a rate of 1.41% per year. Neither HIV status nor nutritional supplementations were found to affect the pharmacokinetics of these drugs in our cohort of patients.
Conflict of interest statement
Figures



References
-
- Wada M, Yoshiyama T, Ogata H, Ito K, Mizutani S, Sugita H. [Six-months chemotherapy (2HRZS or E/4HRE) of new cases of pulmonary tuberculosis—six year experiences on its effectiveness, toxicity, and acceptability]. Kekkaku. 1999;74(4):353–60. Epub 1999/06/04. . - PubMed
-
- Treatment of tuberculosis and tuberculosis infection in adults and children. American Thoracic Society. Monaldi Arch Chest Dis. 49(4):327–45. Epub 1994/09/01. . - PubMed
-
- World Health Organization. Global tuberculosis report 2013 Geneva, Switzerland: World Health Organization; 2013.
-
- Ministry of Health and Social welfare. Manual of the national tuberculosis and leprosy programme in Tanzania Dar es Salaam: 2013 [cited 2014 30 November]. Sixth:[Available from: ntlp.go.tz/index.php?option=com_phocadownload&view…
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
