

Breast Tumor Prognostic Characteristics and Biennial vs Annual Mammography, Age, and Menopausal Status
- PMID: 26501844
- PMCID: PMC4644100
- DOI: 10.1001/jamaoncol.2015.3084
Breast Tumor Prognostic Characteristics and Biennial vs Annual Mammography, Age, and Menopausal Status
Abstract
Importance: Screening mammography intervals remain under debate in the United States.
Objective: To compare the proportion of breast cancers with less vs more favorable prognostic characteristics in women screening annually vs biennially by age, menopausal status, and postmenopausal hormone therapy (HT) use.
Design, setting, and participants: This was a study of a prospective cohort from 1996 to 2012 at Breast Cancer Surveillance Consortium facilities. A total of 15,440 women ages 40 to 85 years with breast cancer diagnosed within 1 year of an annual or within 2 years of a biennial screening mammogram.
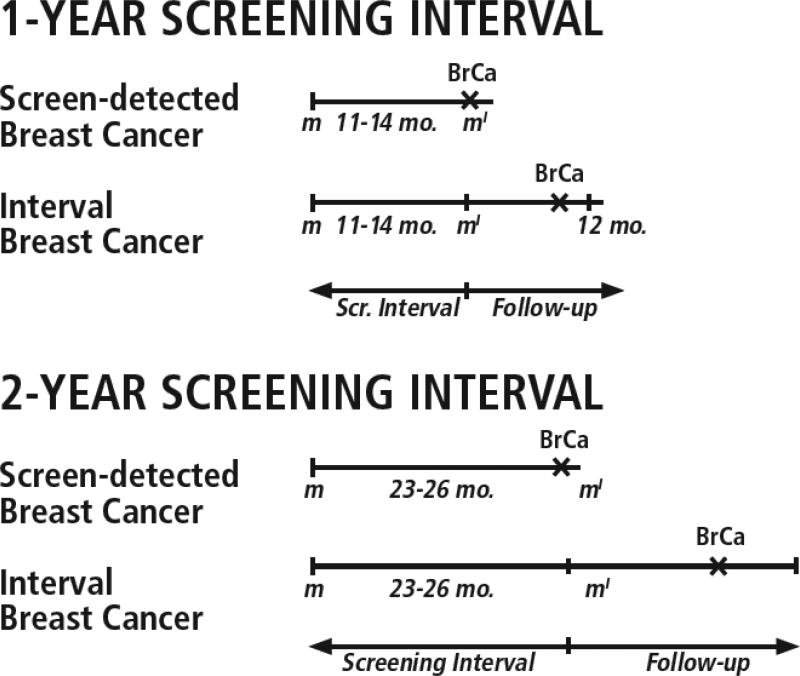
Exposures: We updated previous analyses by using narrower intervals for defining annual (11-14 months) and biennial (23-26 months) screening.
Main outcomes and measures: We defined less favorable prognostic characteristics as tumors that were stage IIB or higher, size greater than 15 mm, positive nodes, and any 1 or more of these characteristics. We used log-binomial regression to model the proportion of breast cancers with less favorable characteristics following a biennial vs annual screen by 10-year age groups and by menopausal status and current postmenopausal HT use.
Results: Among 15,440 women with breast cancer, most were 50 years or older (13,182 [85.4%]), white (12,063 [78.1%]), and postmenopausal (9823 [63.6%]). Among 2027 premenopausal women (13.1%), biennial screeners had higher proportions of tumors that were stage IIB or higher (relative risk [RR], 1.28 [95% CI, 1.01-1.63]; P=.04), size greater than 15 mm (RR, 1.21 [95% CI, 1.07-1.37]; P=.002), and with any less favorable prognostic characteristic (RR, 1.11 [95% CI, 1.00-1.22]; P=.047) compared with annual screeners. Among women currently taking postmenopausal HT, biennial screeners tended to have tumors with less favorable prognostic characteristics compared with annual screeners; however, 95% CIs were wide, and differences were not statistically significant (for stage 2B+, RR, 1.14 [95% CI, 0.89-1.47], P=.29; size>15 mm, RR, 1.13 [95% CI, 0.98-1.31], P=.09; node positive, RR, 1.18 [95% CI, 0.98-1.42], P=.09; any less favorable characteristic, RR, 1.12 [95% CI, 1.00-1.25], P=.053). The proportions of tumors with less favorable prognostic characteristics were not significantly larger for biennial vs annual screeners among postmenopausal women not taking HT (eg, any characteristic: RR, 1.03 [95% CI, 0.95-1.12]; P=.45), postmenopausal HT users after subdividing by type of hormone use (eg, any characteristic: estrogen+progestogen users, RR, 1.16 [95% CI, 0.91-1.47]; P=.22; estrogen-only users, RR, 1.14 [95% CI, 0.94-1.37]; P=.18), or any 10-year age group (eg, any characteristic: ages 40-49 years, RR, .1.04 [95% CI, 0.94-1.14]; P=.48; ages 50-59 years, RR, 1.03 [95% CI, 0.94-1.12]; P=.58; ages 60-69 years, RR, 1.07 [95% CI, 0.97-1.19]; P=.18; ages 70-85 years, RR, 1.05 [95% CI, 0.94-1.18]; P=.35).
Conclusions and relevance: Premenopausal women diagnosed as having breast cancer following biennial vs annual screening mammography are more likely to have tumors with less favorable prognostic characteristics. Postmenopausal women not using HT who are diagnosed as having breast cancer following a biennial or annual screen have similar proportions of tumors with less favorable prognostic characteristics.
Figures
Comment in
-
Optimizing Mammography Screening Intervals.JAMA. 2015 Oct 20;314(15):1635-6. doi: 10.1001/jama.2015.13149. JAMA. 2015. PMID: 26501538 No abstract available.
-
Measuring the Effectiveness of Mammography.JAMA Oncol. 2015 Nov;1(8):1037-8. doi: 10.1001/jamaoncol.2015.3286. JAMA Oncol. 2015. PMID: 26501739 No abstract available.
References
-
- U.S. Preventive Task Force Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716–726. - PubMed
-
- Smith RA, Brooks D, Cokkinides V, Saslow D, Brawley OW. Cancer screening in the United States, 2013: a review of current American Cancer Society guidelines, current issues in cancer screening, and new guidance on cervical cancer screening and lung cancer screening. CA Cancer J Clin. 2013 Mar-Apr;63(2):88–105. - PubMed
-
- Breast cancer screening. Obstet Gynecol. 2011 Aug;118(2 Pt 1):372–382. Practice bulletin no. 122. - PubMed
-
- Bevers TB, Anderson BO, Bonaccio E, et al. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. Journal of the National Comprehensive Cancer Network : JNCCN. 2009 Nov;7(10):1060–1096. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
