

Objective Structured Assessments of Technical Skills (OSATS) Does Not Assess the Quality of the Surgical Result Effectively
- PMID: 26502107
- PMCID: PMC4773332
- DOI: 10.1007/s11999-015-4603-4
Objective Structured Assessments of Technical Skills (OSATS) Does Not Assess the Quality of the Surgical Result Effectively
Abstract
Background: Performance assessment in skills training is ideally based on objective, reliable, and clinically relevant indicators of success. The Objective Structured Assessment of Technical Skill (OSATS) is a reliable and valid tool that has been increasingly used in orthopaedic skills training. It uses a global rating approach to structure expert evaluation of technical skills with the experts working from a list of operative competencies that are each rated on a 5-point Likert scale anchored by behavioral descriptors. Given the observational nature of its scoring, the OSATS might not effectively assess the quality of surgical results.
Questions/purposes: (1) Does OSATS scoring in an intraarticular fracture reduction training exercise correlate with the quality of the reduction? (2) Does OSATS scoring in a cadaveric extraarticular fracture fixation exercise correlate with the mechanical integrity of the fixation?
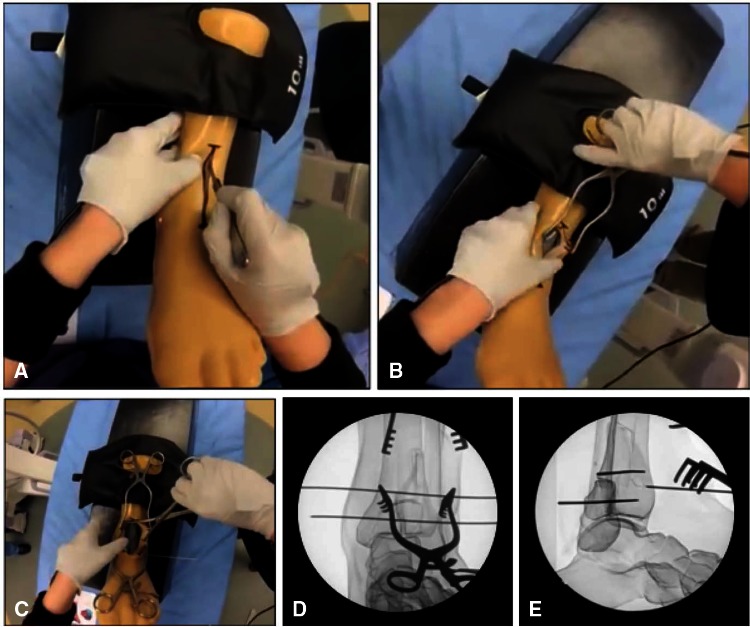
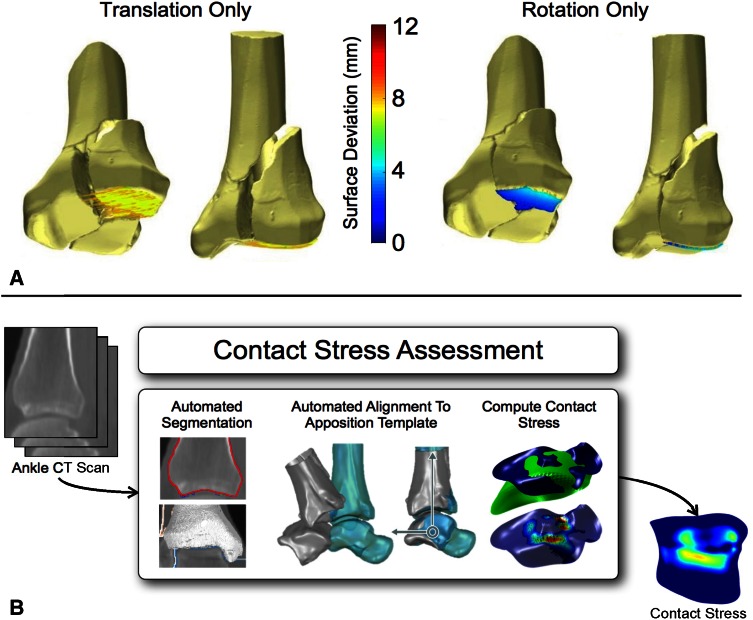
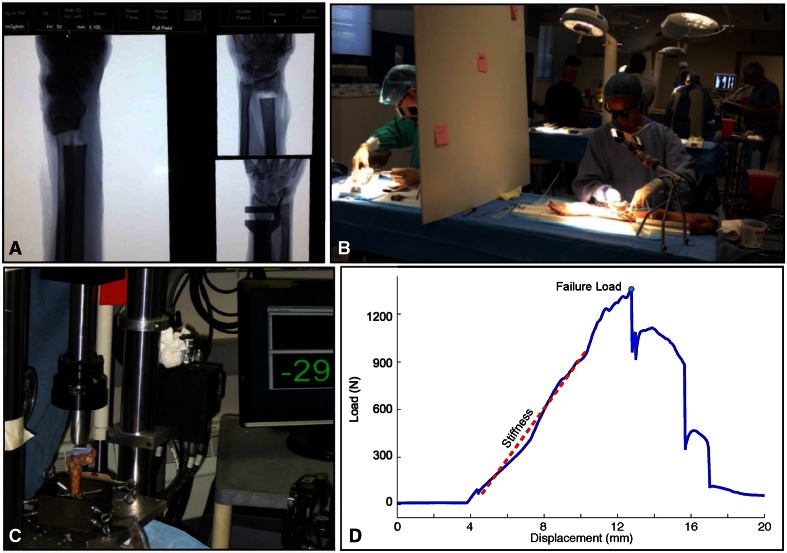
Methods: Orthopaedic residents at the University of Iowa (six postgraduate year [PGY]-1s) and at the University of Minnesota (seven PGY-1s and eight PGY-2s) undertook a skills training exercise that involved reducing a simulated intraarticular fracture under fluoroscopic guidance. Iowa residents participated three times during 1 month, and Minnesota residents participated twice with 1 month between their two sessions. A fellowship-trained orthopaedic traumatologist rated each performance using a modified OSATS scoring scheme. The quality of the articular reduction obtained was then directly measured. Regression analysis was performed between OSATS scores and two metrics of articular reduction quality: articular surface deviation and estimated contact stress. Another skills training exercise involved fixing a simulated distal radius fracture in a cadaveric specimen. Thirty residents, distributed across four PGY classes (PGY-2 and PGY-3, n = 8 each; PGY-4 and PGY-5, n = 7 each), simultaneously completed the exercise at individual stations. One of three faculty hand surgeons independently scored each performance using a validated OSATS scoring system. The mechanical integrity of each fixation construct was then assessed in a materials testing machine. Regression analysis was performed between OSATS scores and two metrics of fixation integrity: stiffness and failure load.
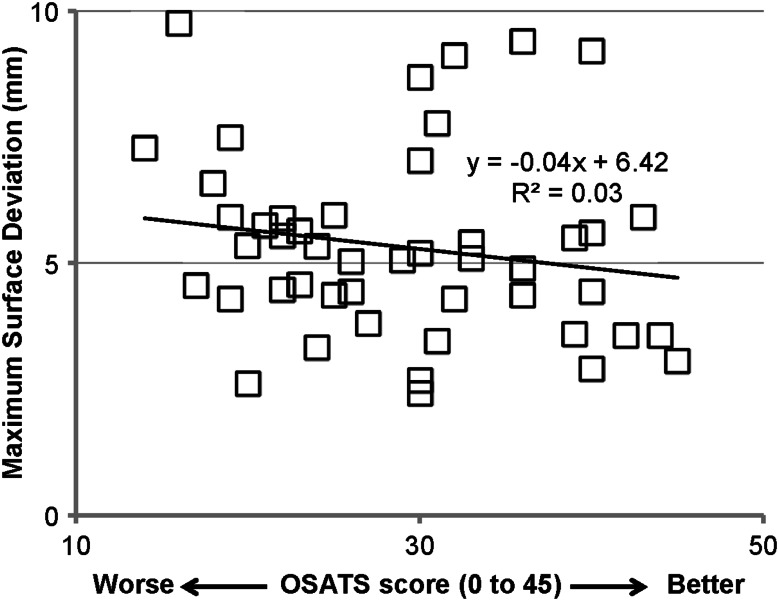
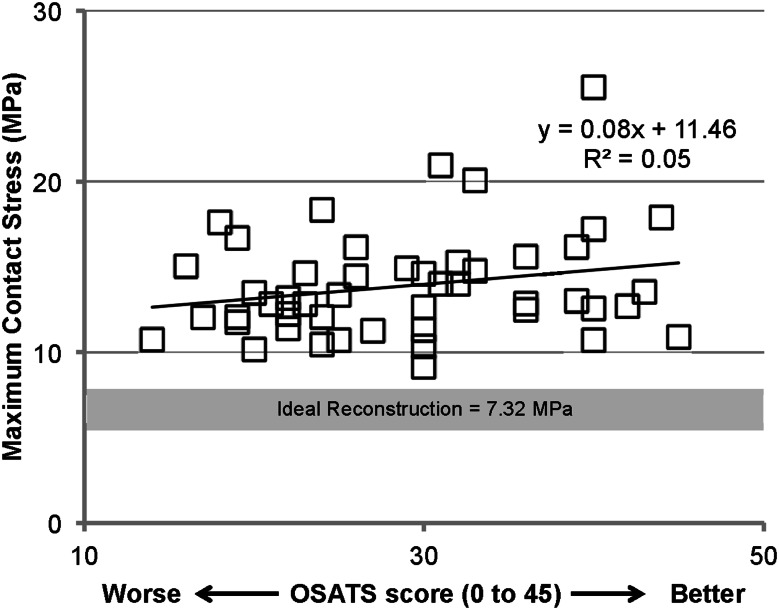
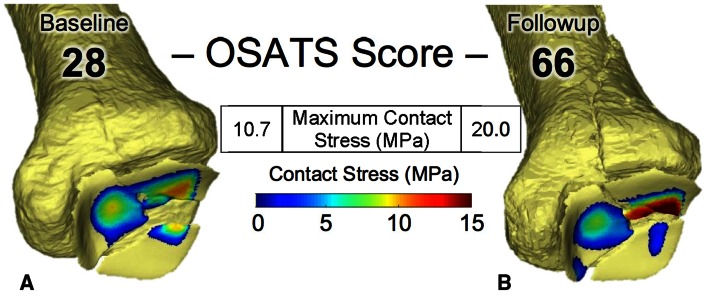
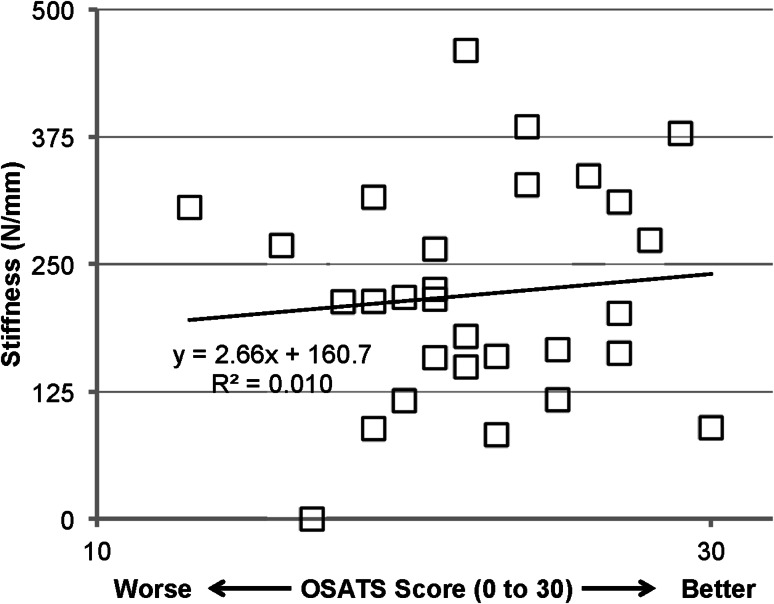
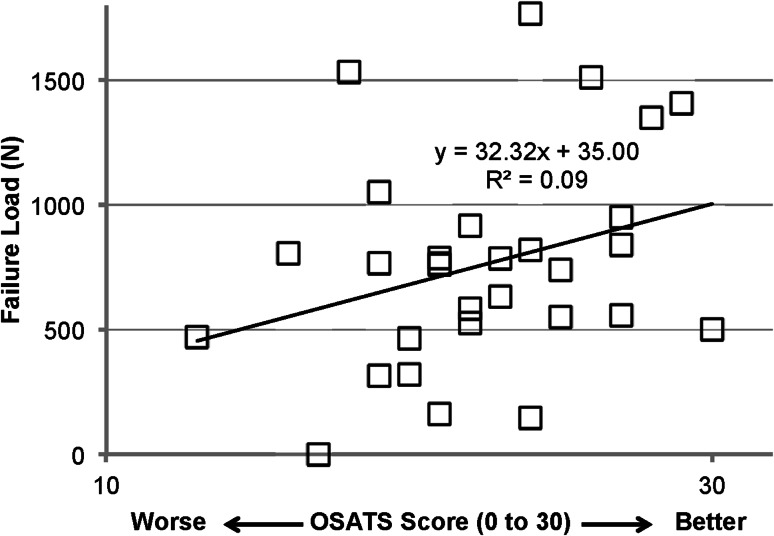
Results: In the intraarticular fracture model, OSATS scores did not correlate with articular reduction quality (maximum surface deviations: R = 0.17, p = 0.25; maximum contact stress: R = 0.22, p = 0.13). Similarly in the cadaveric extraarticular fracture model, OSATS scores did not correlate with the integrity of the mechanical fixation (stiffness: R = 0.10, p = 0.60; failure load: R = 0.30, p = 0.10).
Conclusions: OSATS scoring methods do not effectively assess the quality of the surgical result. Efforts must be made to incorporate assessment metrics that reflect the quality of the surgical result.
Clinical relevance: New objective, reliable, and clinically relevant measures of the quality of the surgical result obtained by a trainee are urgently needed. For intraarticular fracture reduction and extraarticular fracture fixation, direct physical measurement of reduction quality and of mechanical integrity of fixation, respectively, meet this need.
Figures
Comment in
-
Editor's Spotlight/Take 5: Objective Structured Assessments of Technical Skills (OSATS) Does Not Assess the Quality of the Surgical Result Effectively.Clin Orthop Relat Res. 2016 Apr;474(4):871-3. doi: 10.1007/s11999-015-4677-z. Epub 2016 Jan 4. Clin Orthop Relat Res. 2016. PMID: 26728515 Free PMC article. No abstract available.
Similar articles
-
Editor's Spotlight/Take 5: Objective Structured Assessments of Technical Skills (OSATS) Does Not Assess the Quality of the Surgical Result Effectively.Clin Orthop Relat Res. 2016 Apr;474(4):871-3. doi: 10.1007/s11999-015-4677-z. Epub 2016 Jan 4. Clin Orthop Relat Res. 2016. PMID: 26728515 Free PMC article. No abstract available.
-
Do orthopaedic fracture skills courses improve resident performance?Injury. 2015 Apr;46(4):547-51. doi: 10.1016/j.injury.2014.10.061. Epub 2014 Nov 18. Injury. 2015. PMID: 25476015
-
Cognitive and Psychomotor Entrustable Professional Activities: Can Simulators Help Assess Competency in Trainees?Clin Orthop Relat Res. 2016 Apr;474(4):926-34. doi: 10.1007/s11999-015-4553-x. Clin Orthop Relat Res. 2016. PMID: 26394640 Free PMC article.
-
Surgical Coaching from Head-Mounted Video in the Training of Fluoroscopically Guided Articular Fracture Surgery.J Bone Joint Surg Am. 2015 Jun 17;97(12):1031-9. doi: 10.2106/JBJS.N.00748. J Bone Joint Surg Am. 2015. PMID: 26085538 Review.
-
Objective Assessment of General Surgery Residents Followed by Remediation.J Surg Educ. 2016 Nov-Dec;73(6):e71-e76. doi: 10.1016/j.jsurg.2016.07.002. Epub 2016 Jul 29. J Surg Educ. 2016. PMID: 27476792 Review.
Cited by
-
Advancing Simulation-Based Orthopaedic Surgical Skills Training: An Analysis of the Challenges to Implementation.Adv Orthop. 2019 Sep 2;2019:2586034. doi: 10.1155/2019/2586034. eCollection 2019. Adv Orthop. 2019. PMID: 31565441 Free PMC article. Review.
-
Development of a certification examination for orthopedic sports medicine fellows.Can J Surg. 2020 Mar 6;63(2):E110-E117. doi: 10.1503/cjs.015418. Can J Surg. 2020. PMID: 32142243 Free PMC article.
-
A Vision for Using Simulation & Virtual Coaching to Improve the Community Practice of Orthopedic Trauma Surgery.Iowa Orthop J. 2020;40(1):25-34. Iowa Orthop J. 2020. PMID: 32742205 Free PMC article.
-
Analyses of Orthopaedic Surgery Residency Interviews.JB JS Open Access. 2023 Jan 19;8(1):e22.00084. doi: 10.2106/JBJS.OA.22.00084. eCollection 2023 Jan-Mar. JB JS Open Access. 2023. PMID: 36698983 Free PMC article. Review.
-
Construct and face validity of the educational computer-based environment (ECE) assessment scenarios for basic endoneurosurgery skills.Surg Endosc. 2017 Nov;31(11):4485-4495. doi: 10.1007/s00464-017-5502-4. Epub 2017 Apr 7. Surg Endosc. 2017. PMID: 28389794
References
-
- Buckwalter JA, Brown TD. Joint injury, repair, and remodeling: roles in post-traumatic osteoarthritis. Clin Orthop Relat Res. 2004;423:7–16. doi: 10.1097/01.blo.0000131638.81519.de. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
