

Ulnar Collateral Ligament Reconstruction: Anatomy, Indications, Techniques, and Outcomes
- PMID: 26502444
- PMCID: PMC4622381
- DOI: 10.1177/1941738115607208
Ulnar Collateral Ligament Reconstruction: Anatomy, Indications, Techniques, and Outcomes
Abstract
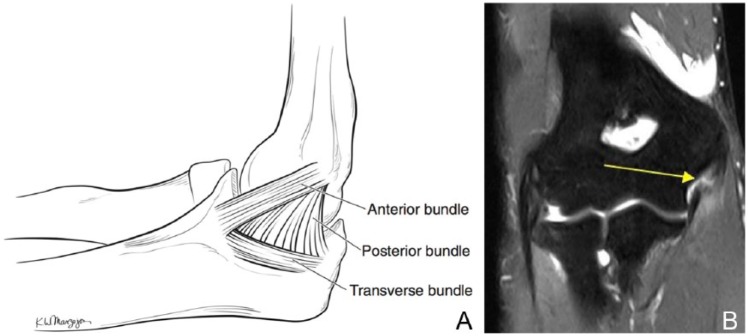
Context: Ulnar collateral ligament (UCL) injuries lead to pain and loss of performance in the thrower's elbow. Ulnar collateral ligament reconstruction (UCLR) is a reliable treatment option for the symptomatic, deficient UCL. Injury to the UCL usually occurs because of chronic accumulation of microtrauma, although acute ruptures occur and an acute-on-chronic presentation is also common.
Evidence acquisition: Computerized databases, references from pertinent articles, and research institutions were searched for all studies using the search terms ulnar collateral ligament from 1970 until 2015.
Study design: Clinical review.
Level of evidence: Level 5.
Results: All studies reporting outcomes for UCLR are level 4. Most modern fixation methodologies appear to be biomechanically and clinically equivalent. Viable graft choices include ipsilateral palmaris longus tendon autograft, gracilis or semitendinosus autograft, and allograft. Clinical studies report excellent outcomes of UCLR for both recreational and elite level athletes with regard to return to sport and postoperative performance. Complications, although rare, include graft rerupture or attenuation, ulnar nerve symptoms, stiffness, pain, and/or weakness leading to decreased performance.
Conclusion: Injuries to the UCL have become commonplace among pitchers. Nonoperative treatment should be attempted, but the limited studies have not shown promising results. Operative treatment can be performed with several techniques, with retrospective studies showing promising results. Complications include ulnar neuropathy as well as failure to return to sport. Detailed preoperative planning, meticulous surgical technique, and a comprehensive rehabilitation program are essential components to achieving a satisfactory result.
Keywords: Tommy John; biomechanics; elbow; instability; pitcher; surgical management; throwing athlete; ulnar collateral ligament reconstruction.
© 2015 The Author(s).
Conflict of interest statement
The following authors declared potential conflicts of interest: Bernard R. Bach Jr, MD, had grants/grants pending from Arthrex, Conmed, DJO, Ossur, Smith & Nephew, and Tornier and received royalties from SLACK. Nikhil N. Verma, MD, has grants/grants pending from Arthrex, Arthrosurface, DJO, Smith & Nephew, Athletico, and Conmed; receives royalties from Smith & Nephew and Vindico; and has stock/stock options from Omeros, Minivasive, and Cymedica. Charles A. Bush-Joseph, MD, is a paid consultant and lecturer for Arthrex; has grants/grants pending from DJO, Ossur, Smith & Nephew, and Arthrex; and receives royalties from Saunders/Mosby.
Figures


References
-
- Ahmad CS, Grantham WJ, Greiwe RM. Public perceptions of Tommy John surgery. Phys Sportsmed. 2012;40:64-72. - PubMed
-
- Ahmad CS, Lee TQ, ElAttrache NS. Biomechanical evaluation of a new ulnar collateral ligament reconstruction technique with interference screw fixation. Am J Sports Med. 2003;31:332-337. - PubMed
-
- Andrews JR, Timmerman LA. Outcome of elbow surgery in professional baseball players. Am J Sports Med. 1995;23:407-413. - PubMed
-
- Azar FM, Andrews JR, Wilk KE, Groh D. Operative treatment of ulnar collateral ligament injuries of the elbow in athletes. Am J Sports Med. 2000;28:16-23. - PubMed
-
- Bica D, Armen J, Kulas AS, Youngs K, Womack Z. Reliability and precision of stress sonography of the ulnar collateral ligament. J Ultrasound Med. 2015;34:371-376. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
