

Evaluation of the Usefulness of Consensus Definitions of Sarcopenia in Older Men: Results from the Observational Osteoporotic Fractures in Men Cohort Study
- PMID: 26502831
- PMCID: PMC4739621
- DOI: 10.1111/jgs.13788
Evaluation of the Usefulness of Consensus Definitions of Sarcopenia in Older Men: Results from the Observational Osteoporotic Fractures in Men Cohort Study
Erratum in
-
Erratum.J Am Geriatr Soc. 2018 Jul;66(7):1442. doi: 10.1111/jgs.15408. J Am Geriatr Soc. 2018. PMID: 30117569 No abstract available.
Abstract
Objective: To evaluate the associations between definitions of sarcopenia and clinical outcomes and the ability of the definitions to discriminate those with a high likelihood of having these outcomes from those with a low likelihood.
Design: Osteoporotic Fractures in Men Study.
Setting: Six clinical centers.
Participants: Community-dwelling men aged 65 and older (N = 5,934).
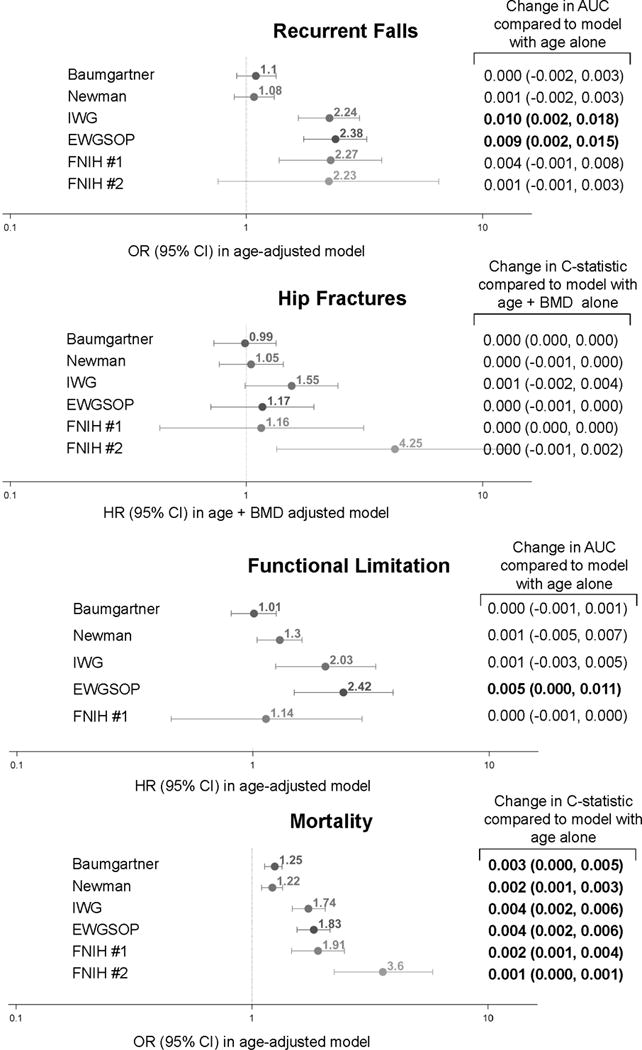
Measurements: Sarcopenia definitions from the International Working Group, European Working Group on Sarcopenia in Older Persons, Foundation for the National Institutes of Health Sarcopenia Project, Baumgartner, and Newman were evaluated. Recurrent falls were defined as two or more self-reported falls in the year after baseline (n = 694, 11.9%). Incident hip fractures (n = 207, 3.5%) and deaths (n = 2,003, 34.1%) were confirmed according to central review of medical records over 9.8 years. Self-reported functional limitations were assessed at baseline and 4.6 years later. Logistic regression or proportional hazards models were used to estimate associations between sarcopenia and falls, hip fractures, and death. The discriminative ability of the sarcopenia definitions (vs reference models) for these outcomes was evaluated using area under the receiver operating characteristic curve or C-statistics. Referent models included age alone for falls, functional limitations and mortality, and age and bone mineral density for hip fractures.
Results: The association between sarcopenia according to the various definitions and risk of falls, functional limitations, and hip fractures was variable; all definitions were associated with greater risk of death, but none of the definitions materially changed discrimination based on the AUC and C-statistic when compared with reference models (change ≤1% in all models).
Conclusion: Sarcopenia definitions as currently constructed did not consistently improve prediction of clinical outcomes in relatively healthy older men.
Keywords: falls; fractures; functional limitation; mortality; sarcopenia.
© 2015, Copyright the Authors Journal compilation © 2015, The American Geriatrics Society.
Conflict of interest statement
Conflict of interest: Dr. Cawthon reports consultancy with Amgen, Eli Lilly and KineMed, and grants to her institution from IMS Health, GlaxoSmithKline, Merck and Amgen for work outside this manuscript. Dr. Ensrud serves as a consultant on a Data Monitoring Committee for Merck Sharpe & Dohme. Dr. Cummings reports consultancy with Eli Lilly and GlaxoSmithKline for work outside this manuscript. Drs. Orwoll, Hoffman, Nevitt, Lee, Lane, Barrett-Connor, Kado, Cauley and Stefanick, and Ms. Blackwell have nothing to disclose.
Figures
References
-
- Muscaritoli M, Anker SD, Argiles J, et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin Nutr. 2010;29:154–159. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
