

Ablative Radiotherapy Doses Lead to a Substantial Prolongation of Survival in Patients With Inoperable Intrahepatic Cholangiocarcinoma: A Retrospective Dose Response Analysis
- PMID: 26503201
- PMCID: PMC4980564
- DOI: 10.1200/JCO.2015.61.3778
Ablative Radiotherapy Doses Lead to a Substantial Prolongation of Survival in Patients With Inoperable Intrahepatic Cholangiocarcinoma: A Retrospective Dose Response Analysis
Erratum in
-
Errata.J Clin Oncol. 2019 Apr 10;37(11):942. doi: 10.1200/JCO.19.00518. J Clin Oncol. 2019. PMID: 30951646 Free PMC article. No abstract available.
Abstract
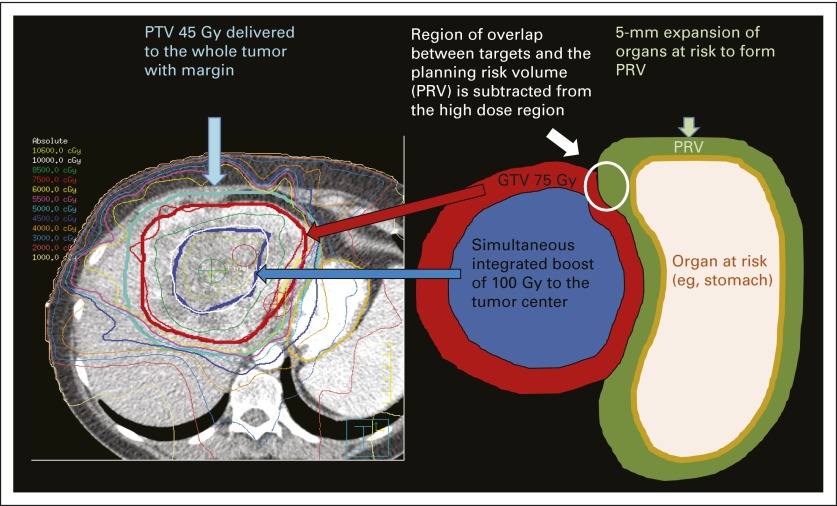
Purpose: Standard therapies for localized inoperable intrahepatic cholangiocarcinoma (IHCC) are ineffective. Advances in radiotherapy (RT) techniques and image guidance have enabled ablative doses to be delivered to large liver tumors. This study evaluated the effects of RT dose escalation in the treatment of IHCC.
Patients and methods: Seventy-nine consecutive patients with inoperable IHCC were identified and treated with definitive RT from 2002 to 2014. At diagnosis, the median tumor size was 7.9 cm (range, 2.2 to 17 cm). Seventy patients (89%) received systemic chemotherapy before RT. RT doses were 35 to 100 Gy (median, 58.05 Gy) in three to 30 fractions for a median biologic equivalent dose (BED) of 80.5 Gy (range, 43.75 to 180 Gy).
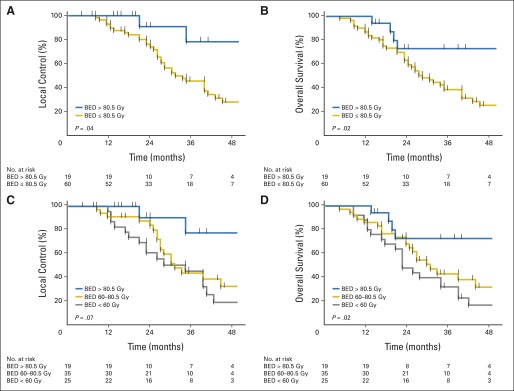
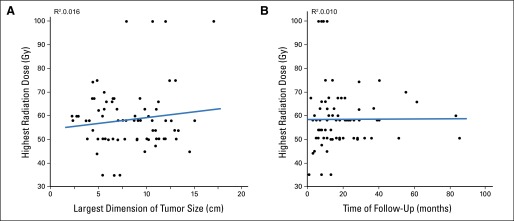
Results: Median follow-up time for patients alive at time of analysis was 33 months (range, 11 to 93 months). Median overall survival (OS) time after diagnosis was 30 months; 3-year OS rate was 44%. Radiation dose was the single most important prognostic factor; higher doses correlated with an improved local control (LC) rate and OS. The 3-year OS rate for patients receiving BED greater than 80.5 Gy was 73% versus 38% for those receiving lower doses (P = .017); 3-year LC rate was significantly higher (78%) after a BED greater than 80.5 Gy than after lower doses (45%, P = .04). BED as a continuous variable significantly affected LC (P = .009) and OS (P = .004). There were no significant treatment-related toxicities.
Conclusion: Delivery of higher doses of RT improves LC and OS in inoperable IHCC. A BED greater than 80.5 Gy seems to be an ablative dose of RT for large IHCCs, with long-term survival rates that compare favorably with resection.
Trial registration: ClinicalTrials.gov NCT02200042.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
Comment in
-
To RCT or Not to RCT: How to Change Practice for Rare Cancers?J Clin Oncol. 2016 Jan 20;34(3):203-4. doi: 10.1200/JCO.2015.63.8767. Epub 2015 Dec 7. J Clin Oncol. 2016. PMID: 26644540 No abstract available.
-
Gastrointestinal Cancers-Changing the Standard for Rectal Cancer and Establishing a New Standard for Liver Tumors.Int J Radiat Oncol Biol Phys. 2016 Jul 1;95(3):930-6. doi: 10.1016/j.ijrobp.2016.02.024. Int J Radiat Oncol Biol Phys. 2016. PMID: 27302509 Free PMC article. No abstract available.
References
-
- Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology. 2001;33:1353–1357. - PubMed
-
- Shaib YH, Davila JA, McGlynn K, et al. Rising incidence of intrahepatic cholangiocarcinoma in the United States: A true increase? J Hepatol. 2004;40:472–477. - PubMed
-
- Vauthey JN, Blumgart LH. Recent advances in the management of cholangiocarcinomas. Semin Liver Dis. 1994;14:109–114. - PubMed
-
- Chou FF, Sheen-Chen SM, Chen YS, et al. Surgical treatment of cholangiocarcinoma. Hepatogastroenterology. 1997;44:760–765. - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
