

Mechanical versus manual chest compressions for out-of-hospital cardiac arrest: a meta-analysis of randomized controlled trials
- PMID: 26503429
- PMCID: PMC4621518
- DOI: 10.1038/srep15635
Mechanical versus manual chest compressions for out-of-hospital cardiac arrest: a meta-analysis of randomized controlled trials
Abstract
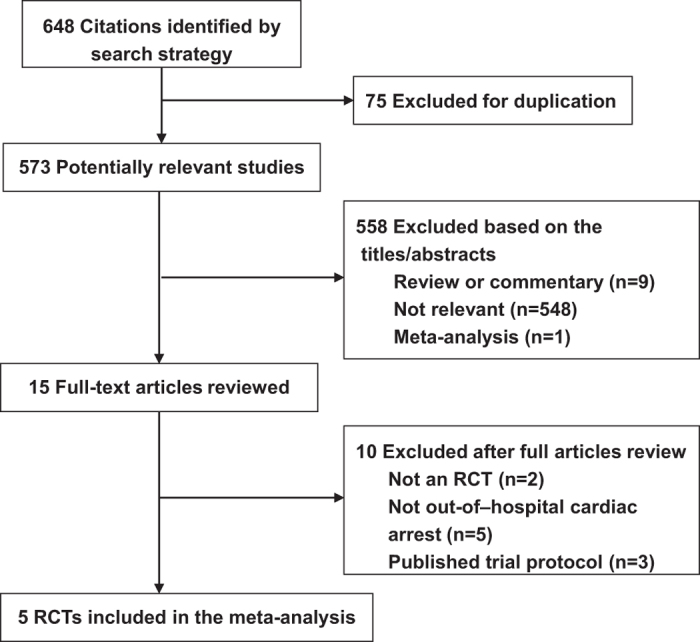
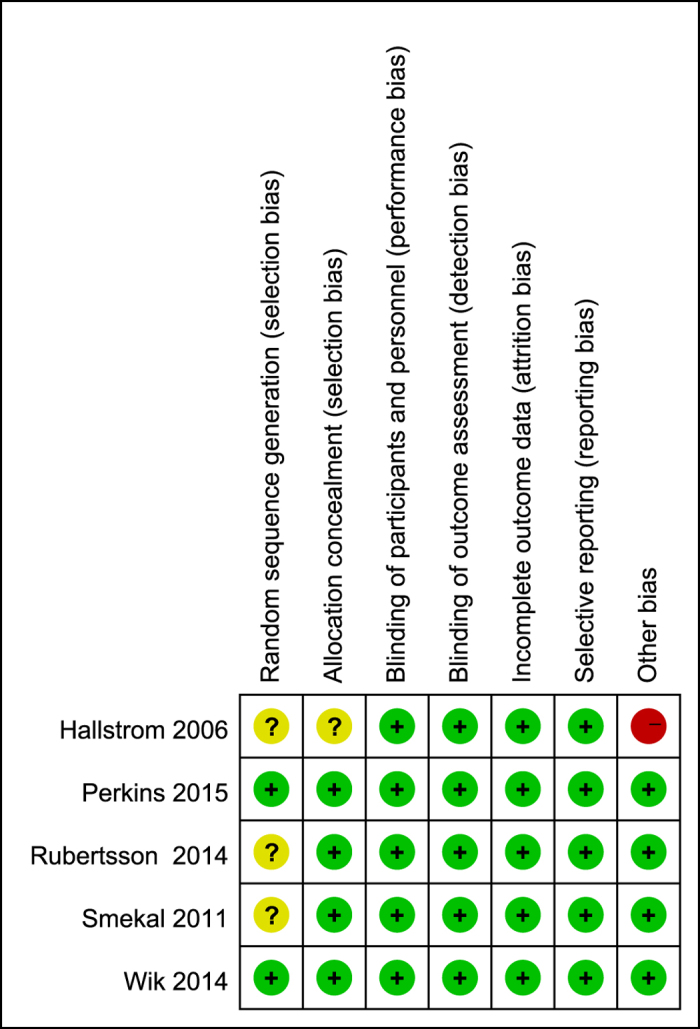
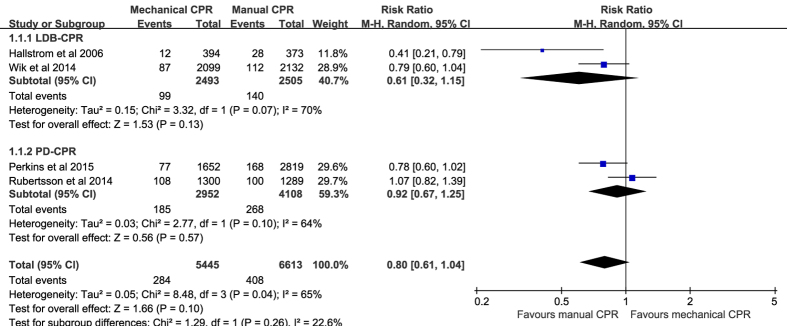
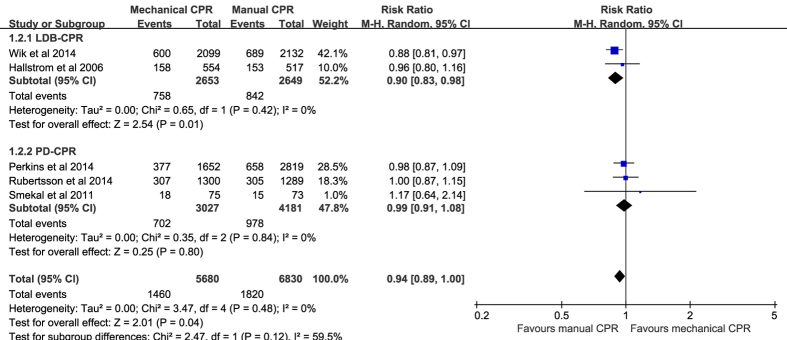
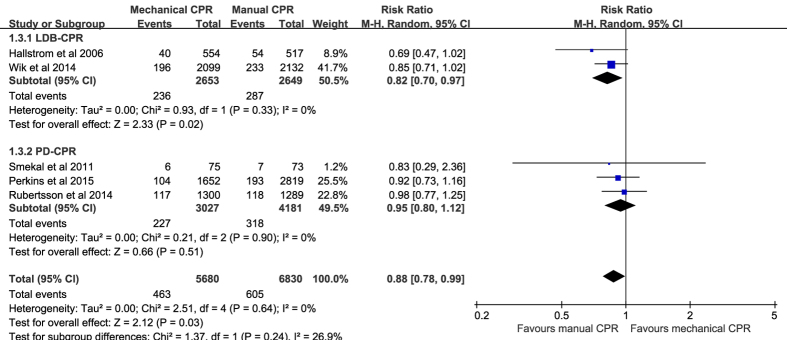
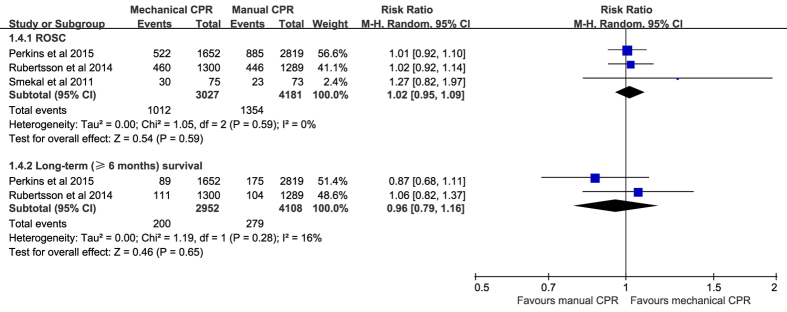
Recent evidence regarding mechanical chest compressions in out-of-hospital cardiac arrest (OHCA) is conflicting. The objective of this study was to perform a meta-analysis of randomized controlled trials (RCTs) to compare the effect of mechanical versus manual chest compressions on resuscitation outcomes in OHCA. PubMed, Embase, the Cochrane Central Register of Controlled Trials, and the ClinicalTrials.gov registry were searched. In total, five RCTs with 12,510 participants were included. Compared with manual chest compressions, mechanical chest compressions did not significantly improve survival with good neurological outcome to hospital discharge (relative risks (RR) 0.80, 95% CI 0.61-1.04, P = 0.10; I(2) = 65%), return of spontaneous circulation (RR 1.02, 95% CI 0.95-1.09, P = 0.59; I(2) = 0%), or long-term (≥6 months) survival (RR 0.96, 95% CI 0.79-1.16, P = 0.65; I(2) = 16%). In addition, mechanical chest compressions were associated with worse survival to hospital admission (RR 0.94, 95% CI 0.89-1.00, P = 0.04; I(2) = 0%) and to hospital discharge (RR 0.88, 95% CI 0.78-0.99, P = 0.03; I(2) = 0%). Based on the current evidence, widespread use of mechanical devices for chest compressions in OHCA cannot be recommended.
Figures
References
-
- Lombardi G., Gallagher J. & Gennis P. Outcome of out-of-hospital cardiac arrest in New York City. The pre-hospital arrest survival evaluation (phase) study. JAMA 271, 678–83 (1994). - PubMed
-
- Young G. Neurologic prognosis after cardiac arrest. New England Journal of Medicine 361, 605–11 (2009). - PubMed
-
- Ewy G. A. Cardiocerebral resuscitation: The new cardiopulmonary resuscitation. Circulation 111, 2134–42 (2005). - PubMed
-
- Stiell I. et al. Health-related quality of life is better for cardiac arrest survivors who received citizen cardiopulmonary resuscitation. Circulation 108, 1939–44 (2003). - PubMed
-
- Rubertsson S. & Karlsten R. Increased cortical cerebral blood flow with lucas; a new device for mechanical chest compressions compared to standard external compressions during experimental cardiopulmonary resuscitation. Resuscitation 65, 357–63 (2005). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
