

Reconstructive laparoscopic prolapse surgery to avoid mesh erosions
- PMID: 26504702
- PMCID: PMC4582496
- DOI: 10.3205/iprs000031
Reconstructive laparoscopic prolapse surgery to avoid mesh erosions
Abstract
Introduction: The objective of the study is to examine the efficacy of the purely laparoscopic reconstructive management of cystocele and rectocele with mesh, to avoid the risk of erosion by the graft material, a well known complication in vaginal mesh surgery.
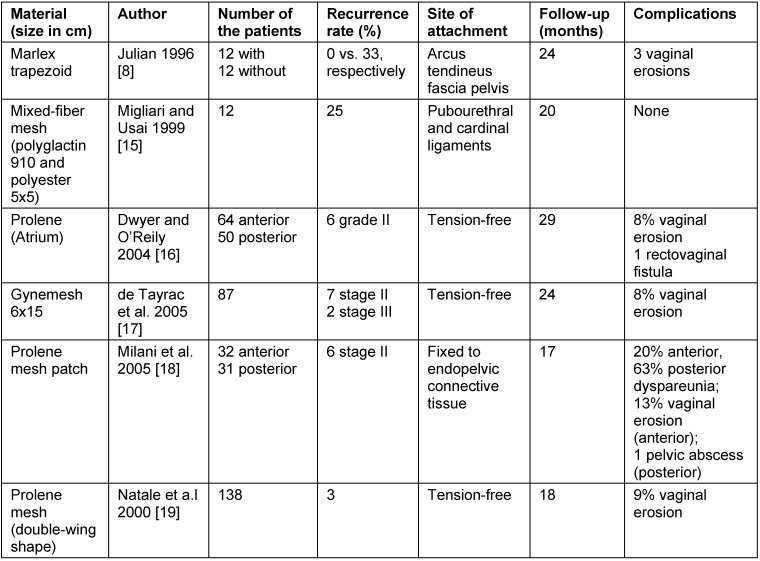
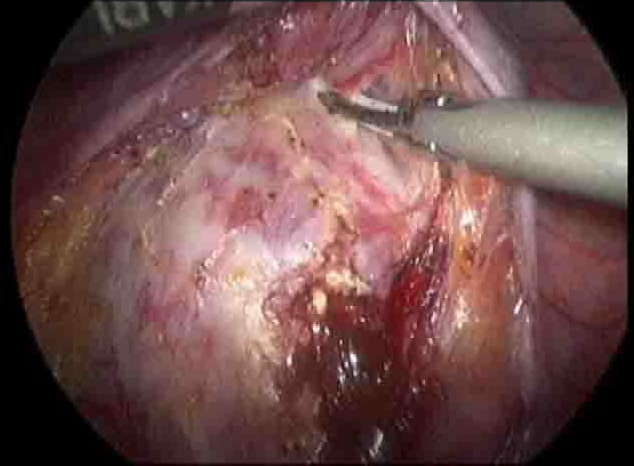
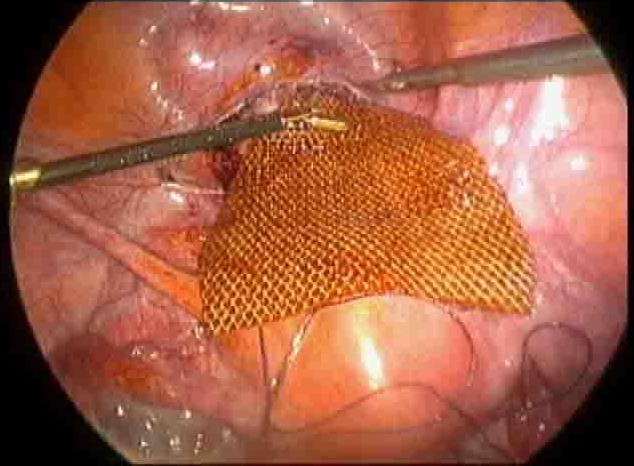
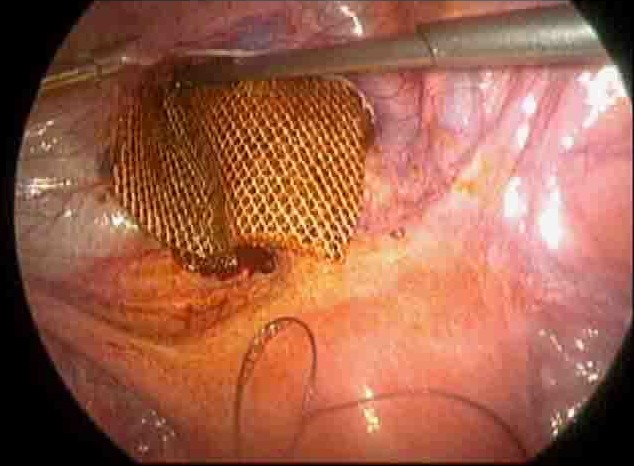
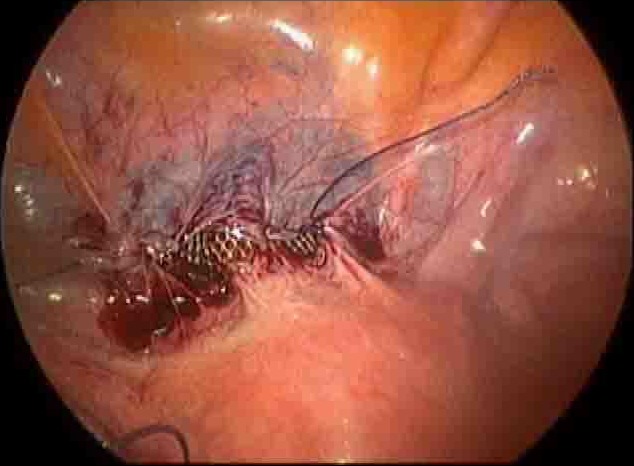
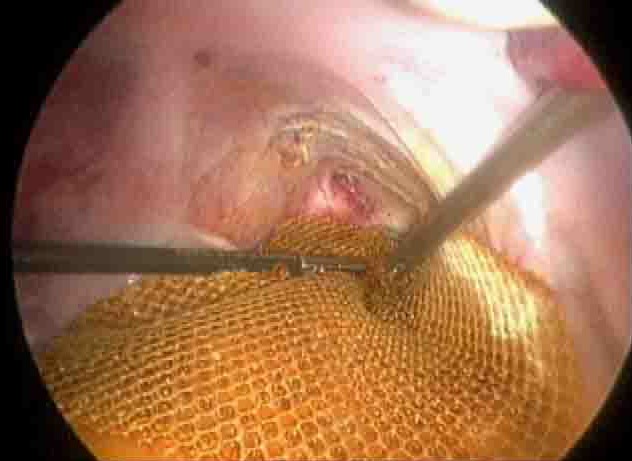
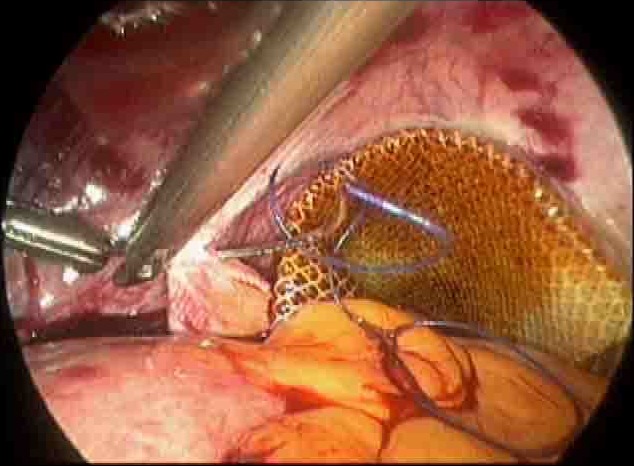
Material and methods: We performed a prospective, single-case, non-randomized study in 325 patients who received laparoscopic reconstructive management of pelvic organe prolaps with mesh. The study was conducted between January 2004 and December 2012 in a private clinic in India. The most common prolapse symptoms were reducible vaginal lump, urinary stress incontinence, constipation and flatus incontinence, sexual dysfunction and dypareunia. The degree e of the prolaps was staged according to POPQ system. The approach was purely laparoscopic and involved the use of polypropylene (Prolene) or polyurethane with activated regenerated cellulose coating (Parietex) mesh.
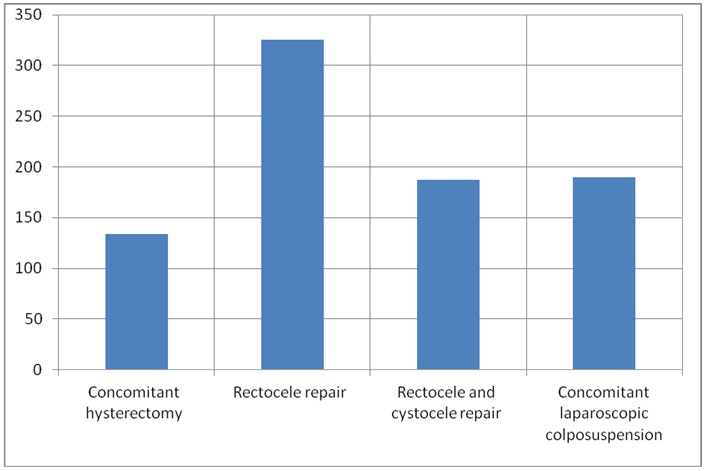
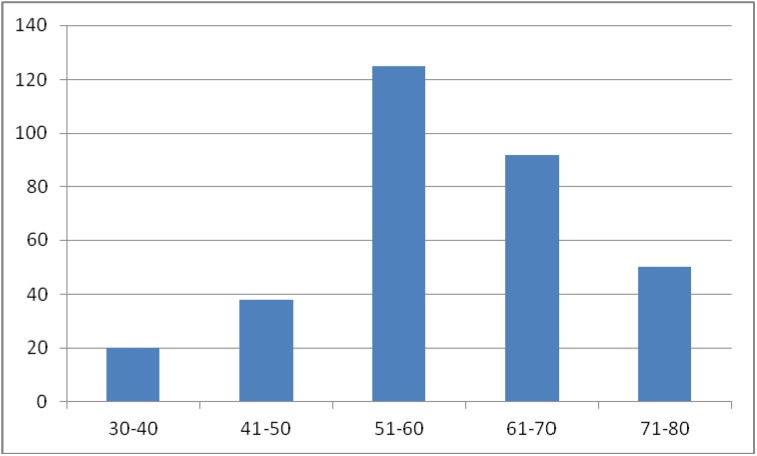
Results: The mean age was 55 (30-80) years and the most of the patients were multiparous (272/325). The patients received a plastic correction of the rectocele only (138 cases), a cystocele and rectocele (187 cases) with mesh. 132 patients had a concomitant total hysterectomy; in 2 cases a laparoscopic supracervical hysterectomy was performed and 190 patients had a laparoscopic colposuspension. The mean operation time was 82.2 (60-210) minutes. The mean follow up was 3.4 (3-5) years. Urinary retention developed in 1 case, which required a new laparoscopical intervention. Bladder injury, observed in the same case was in one session closed with absorbable suture. There were four recurrences of the rectocele, receiving a posterior vaginal colporrhaphy. Erosions of the mesh were not reported or documented.
Conclusion: The pure laparoscopic reconstructive management of the cystocele and rectocele with mesh seems to be a safe and effective surgical procedure potentially avoiding the risk of mesh erosions.
Einleitung: Das Studienziel ist die Überprüfung der Sicherheit und Effizienz der rein laparoskopisch-rekonstruktiven Operation der Cysto- und Rektocele mittels Netz, um das Risiko der Mesh-Erosion, einer bekannten Komplikation bei der vaginalen Chirurgie, zu vermeiden.Material und Methodik: Wir führten eine prospektive, nicht randomisierte Single-Case-Studie mit 325 Patientinnen durch, die einen laparoskopisch-rekonstruktiven Eingriff bei einem Beckenorgan-Vorfall mittels Netzeinlage erhielten. Die Studie wurde zwischen Januar 2004 und Dezember 2012 in einer Privatklinik in Indien durchgeführt. Die möglichen klinischen Symptome bei Prolaps sind reponierbare vaginale Vorwölbung, Stressharninkontinenz, Stuhl- und Windinkontinenz sowie Dyspareunie. Der Grad des Prolapses wurde mittels POPQ-System eingestuft. Die Technik war rein laparoskopisch und beinhaltete den Gebrauch von Polypropylene- oder Polyurethane-Mesh mit aktivierter regenerierter Cellulose-Oberfläche. Ergebnisse: Der Altersdurchschnitt betrug 55 (30–80) Jahre und die meisten Patientinnen waren multipara (275/325). In 138 Fällen erhielten die Patientinnen eine plastische Korrektur der Rektocele und in 187 Fällen einer Korrektur von Cysto- und Rektocele mittels Netzeinlage. 132 Patientinnen hatten eine gleichzeitige totale Hysterektomie, in 2 Fällen wurde eine laparoskopische supracervikale Hysterektomie durchgeführt und 190 Patientinnen erhielten eine laparoskopische Kolposuspension. Die durchschnittliche Operationsdauer betrug 82,2 (60–210) Min. Die durchschnittliche Dauer des Follow-up betrug 3,4 (3–5) Jahre. 1 Fall mit Harnverhalt wurde postoperativ identifiziert und erneut laparoskopisch behandelt. Eine Blasenläsion, die im gleichen Fall auffiel, wurde in der gleichen Sitzung mit resorbierbarem Nahtmaterial geschlossen. Es zeigten sich vier Rezidive der Rektocele, die durch eine hintere vaginale Kolporrhaphie behandelt wurden. Es wurden keinerlei Mesh-Erosionen berichtet oder dokumentiert. Schlussfolgerung: Die reine laparoskopisch-rekonstruktive Operation der Cysto- und Rektocele mittels Netz erscheint als eine sichere und effiziente chirurgische Methode, um das potenzielle Risiko von Mesh-Erosionen bei der vaginalen Chirurgie zu vermeiden. Weitere randomisierte Studien sollten durchgeführt werden, um diese Ergebnisse zu bestätigen.
Keywords: mesh surgery; minimally invasive access; reconstructive prolapse repair.
Figures

Similar articles
-
Laparoscopic management of uterine prolapse with cystocele and rectocele using "Gynemesh PS".J Laparoendosc Adv Surg Tech A. 2008 Feb;18(1):93-8. doi: 10.1089/lap.2006.0026. J Laparoendosc Adv Surg Tech A. 2008. PMID: 18266583
-
[Long-term review on posterior colporrhaphy with levator ani muscles plication and incorporating a Vypro II mesh].Ceska Gynekol. 2009 Aug;74(4):282-5. Ceska Gynekol. 2009. PMID: 20564983 Czech.
-
[Prolene mesh sling in the treatment of stress urinary incontinence. Integral treatment of pelvic floor anomalies. Long-term results].Arch Esp Urol. 2002 Nov;55(9):1057-74. Arch Esp Urol. 2002. PMID: 12564066 Clinical Trial. Spanish.
-
Surgical management of pelvic organ prolapse in women: a short version Cochrane review.Neurourol Urodyn. 2008;27(1):3-12. doi: 10.1002/nau.20542. Neurourol Urodyn. 2008. PMID: 18092333 Review.
-
The use of graft materials in vaginal pelvic floor surgery.Int J Gynaecol Obstet. 2006 Mar;92(3):279-88. doi: 10.1016/j.ijgo.2005.11.005. Epub 2006 Jan 19. Int J Gynaecol Obstet. 2006. PMID: 16426613 Review.
References
-
- Swift S, Woodman P, O'Boyle A, Kahn M, Valley M, Bland D, Wang W, Schaffer J. Pelvic Organ Support Study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol. 2005 Mar;192(3):795–806. doi: 10.1016/j.ajog.2004.10.602. Available from: http://dx.doi.org/10.1016/j.ajog.2004.10.602. - DOI - DOI - PubMed
-
- Lee U, Raz S. Emerging concepts for pelvic organ prolapse surgery: What is cure? Curr Urol Rep. 2011 Feb;12(1):62–67. doi: 10.1007/s11934-010-0160-2. Available from: http://dx.doi.org/10.1007/s11934-010-0160-2. - DOI - DOI - PMC - PubMed
-
- Banerjee C, Noé KG. Endoscopic cystocele surgery: lateral repair with combined suture/mesh technique. J Endourol. 2010 Oct;24(10):1565–1569. doi: 10.1089/end.2010.0096. Available from: http://dx.doi.org/10.1089/end.2010.0096. - DOI - DOI - PubMed
-
- Granese R, Candiani M, Perino A, Romano F, Cucinella G. Laparoscopic sacrocolpopexy in the treatment of vaginal vault prolapse: 8 years experience. Eur J Obstet Gynecol Reprod Biol. 2009 Oct;146(2):227–231. doi: 10.1016/j.ejogrb.2009.06.013. Available from: http://dx.doi.org/10.1016/j.ejogrb.2009.06.013. - DOI - DOI - PubMed
-
- Boyles SH, Weber AM, Meyn L. Procedures for pelvic organ prolapse in the United States, 1979-1997. Am J Obstet Gynecol. 2003 Jan;188(1):108–115. doi: 10.1067/mob.2003.101. Available from: http://dx.doi.org/10.1067/mob.2003.101. - DOI - DOI - PubMed
LinkOut - more resources
Full Text Sources
