

Effects of rhBMP-2 on Sandblasted and Acid Etched Titanium Implant Surfaces on Bone Regeneration and Osseointegration: Spilt-Mouth Designed Pilot Study
- PMID: 26504807
- PMCID: PMC4609358
- DOI: 10.1155/2015/459393
Effects of rhBMP-2 on Sandblasted and Acid Etched Titanium Implant Surfaces on Bone Regeneration and Osseointegration: Spilt-Mouth Designed Pilot Study
Abstract
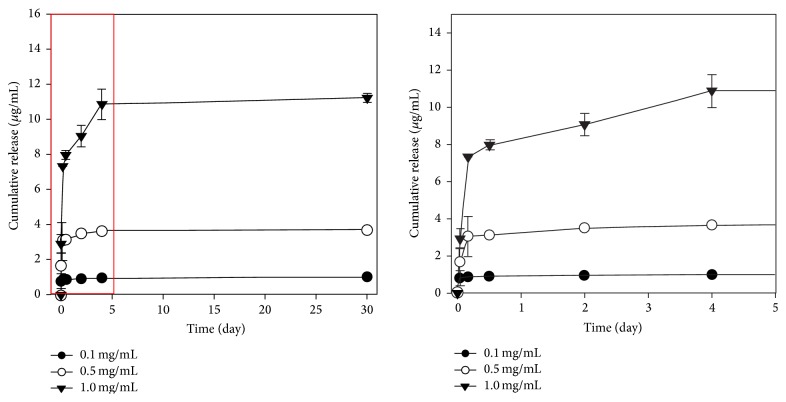
This study was conducted to evaluate effects of rhBMP-2 applied at different concentrations to sandblasted and acid etched (SLA) implants on osseointegration and bone regeneration in a bone defect of beagle dogs as pilot study using split-mouth design. Methods. For experimental groups, SLA implants were coated with different concentrations of rhBMP-2 (0.1, 0.5, and 1 mg/mL). After assessment of surface characteristics and rhBMP-2 releasing profile, the experimental groups and untreated control groups (n = 6 in each group, two animals in each group) were placed in split-mouth designed animal models with buccal open defect. At 8 weeks after implant placement, implant stability quotients (ISQ) values were recorded and vertical bone height (VBH, mm), bone-to-implant contact ratio (BIC, %), and bone volume (BV, %) in the upper 3 mm defect areas were measured. Results. The ISQ values were highest in the 1.0 group. Mean values of VBH (mm), BIC (%), and BV (%) were greater in the 0.5 mg/mL and 1.0 mg/mL groups than those in 0.1 and control groups in buccal defect areas. Conclusion. In the open defect area surrounding the SLA implant, coating with 0.5 and 1.0 mg/mL concentrations of rhBMP-2 was more effective, compared with untreated group, in promoting bone regeneration and osseointegration.
Figures






Similar articles
-
Bone regeneration in dehiscence-type defects at chemically modified (SLActive) and conventional SLA titanium implants: a pilot study in dogs.J Clin Periodontol. 2007 Jan;34(1):78-86. doi: 10.1111/j.1600-051X.2006.01008.x. Epub 2006 Nov 24. J Clin Periodontol. 2007. PMID: 17137467
-
Bone formation at porous titanium implants coated with multiple layers of recombinant human bone morphogenetic protein-2 cDNA plasmid in the posterior mandible in dogs.Int J Oral Maxillofac Implants. 2013 Nov-Dec;28(6):1648-54. doi: 10.11607/jomi.3132. Int J Oral Maxillofac Implants. 2013. PMID: 24278934
-
Effects of different rhBMP-2 release profiles in defect areas around dental implants on bone regeneration.Biomed Mater. 2015 Jul 13;10(4):045007. doi: 10.1088/1748-6041/10/4/045007. Biomed Mater. 2015. PMID: 26165987
-
Tissue engineering with recombinant human bone morphogenetic protein-2 for alveolar augmentation and oral implant osseointegration: experimental observations and clinical perspectives.Clin Implant Dent Relat Res. 2005;7(2):112-9. doi: 10.1111/j.1708-8208.2005.tb00054.x. Clin Implant Dent Relat Res. 2005. PMID: 15996358 Review.
-
Bioactive Surfaces vs. Conventional Surfaces in Titanium Dental Implants: A Comparative Systematic Review.J Clin Med. 2020 Jun 29;9(7):2047. doi: 10.3390/jcm9072047. J Clin Med. 2020. PMID: 32610687 Free PMC article. Review.
Cited by
-
Effectiveness of biomolecule-based bioactive surfaces, on os-seointegration of titanium dental implants: A systematic review and meta-analysis of in vivo studies.Front Bioeng Biotechnol. 2022 Sep 26;10:986112. doi: 10.3389/fbioe.2022.986112. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 36225604 Free PMC article.
-
Integrated analysis of lncRNA-mRNA networks associated with an SLA titanium surface reveals the potential role of HIF1A-AS1 in bone remodeling.RSC Adv. 2020 Jun 2;10(35):20972-20990. doi: 10.1039/d0ra01242d. eCollection 2020 May 27. RSC Adv. 2020. PMID: 35517763 Free PMC article.
-
Dental implant bioactive surface modifications and their effects on osseointegration: a review.Biomark Res. 2016 Dec 14;4:24. doi: 10.1186/s40364-016-0078-z. eCollection 2016. Biomark Res. 2016. PMID: 27999672 Free PMC article. Review.
-
Assessment of Low-Dose rhBMP-2 and Vacuum Plasma Treatments on Titanium Implants for Osseointegration and Bone Regeneration.Materials (Basel). 2025 Jul 30;18(15):3582. doi: 10.3390/ma18153582. Materials (Basel). 2025. PMID: 40805462 Free PMC article.
-
Enhanced osseointegration of dental implants with reduced graphene oxide coating.Biomater Res. 2022 Mar 21;26(1):11. doi: 10.1186/s40824-022-00257-7. Biomater Res. 2022. PMID: 35313996 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
