

Melanopsin retinal ganglion cell loss in Alzheimer disease
- PMID: 26505992
- PMCID: PMC4737313
- DOI: 10.1002/ana.24548
Melanopsin retinal ganglion cell loss in Alzheimer disease
Abstract
Objective: Melanopsin retinal ganglion cells (mRGCs) are photoreceptors driving circadian photoentrainment, and circadian dysfunction characterizes Alzheimer disease (AD). We investigated mRGCs in AD, hypothesizing that they contribute to circadian dysfunction.
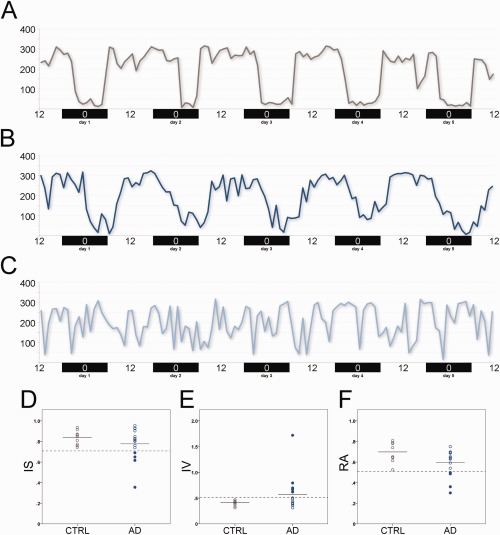
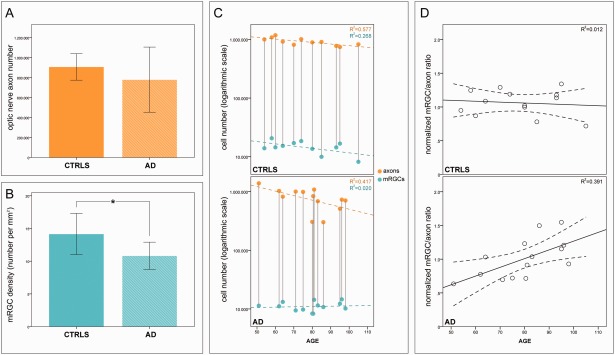
Methods: We assessed retinal nerve fiber layer (RNFL) thickness by optical coherence tomography (OCT) in 21 mild-moderate AD patients, and in a subgroup of 16 we evaluated rest-activity circadian rhythm by actigraphy. We studied postmortem mRGCs by immunohistochemistry in retinas, and axons in optic nerve cross-sections of 14 neuropathologically confirmed AD patients. We coimmunostained for retinal amyloid β (Aβ) deposition and melanopsin to locate mRGCs. All AD cohorts were compared with age-matched controls.
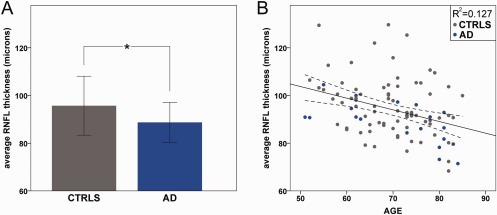
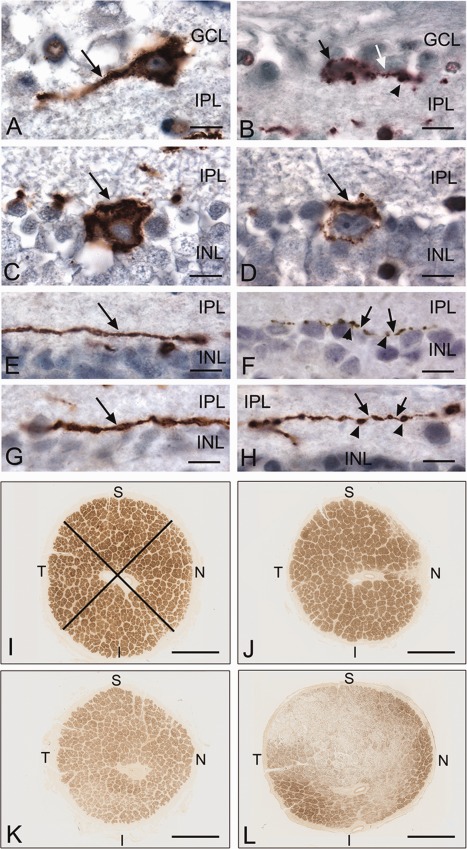
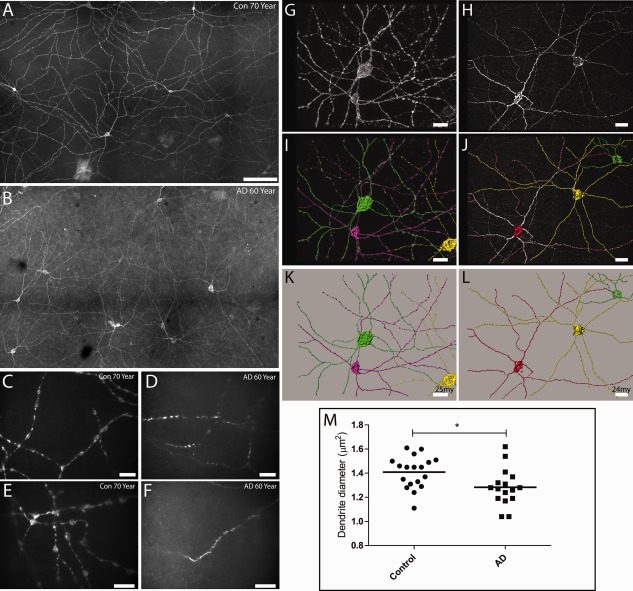
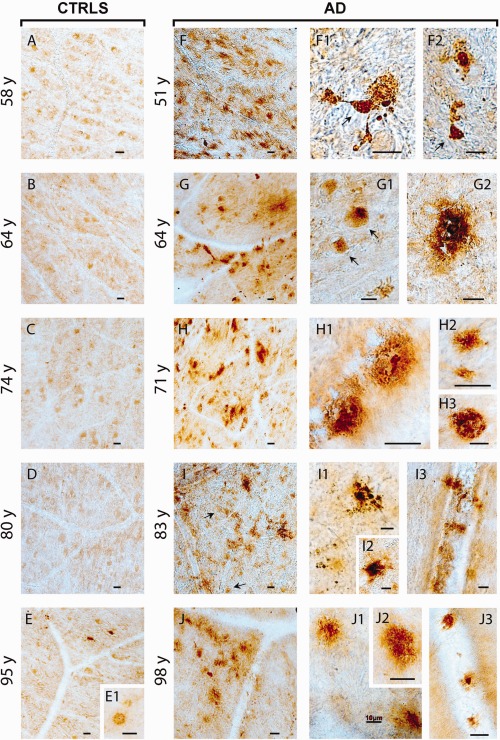
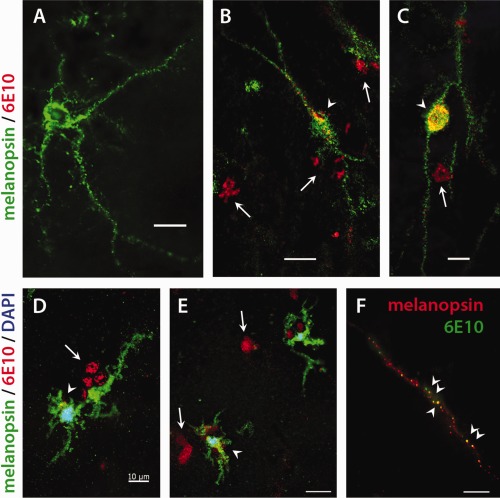
Results: We demonstrated an age-related optic neuropathy in AD by OCT, with a significant reduction of RNFL thickness (p = 0.038), more evident in the superior quadrant (p = 0.006). Axonal loss was confirmed in postmortem AD optic nerves. Abnormal circadian function characterized only a subgroup of AD patients. Sleep efficiency was significantly reduced in AD patients (p = 0.001). We also found a significant loss of mRGCs in postmortem AD retinal specimens (p = 0.003) across all ages and abnormal mRGC dendritic morphology and size (p = 0.003). In flat-mounted AD retinas, Aβ accumulation was remarkably evident inside and around mRGCs.
Interpretation: We show variable degrees of rest-activity circadian dysfunction in AD patients. We also demonstrate age-related loss of optic nerve axons and specifically mRGC loss and pathology in postmortem AD retinal specimens, associated with Aβ deposition. These results all support the concept that mRGC degeneration is a contributor to circadian rhythm dysfunction in AD.
© 2015 American Neurological Association.
Figures
References
-
- Querfurth HW, LaFerla FM. Alzheimer's disease. N Engl J Med 2010;362:329–344. - PubMed
-
- Wu YH, Swaab DF. Disturbance and strategies for reactivation of the circadian rhythm system in aging and Alzheimer's disease. Sleep Med 2007;8:623–636. - PubMed
-
- Hatfield CF, Herbert J, van Someren EJ, et al. Disrupted daily activity/rest cycles in relation to daily cortisol rhythms of home‐dwelling patients with early Alzheimer's dementia. Brain 2004;127:1061–1074. - PubMed
-
- Swaab DF, Fliers E, Partiman TS. The suprachiasmatic nucleus of the human brain in relation to sex, age and senile dementia. Brain Res 1985;342:37–44. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
