

Left ventricular heart failure and pulmonary hypertension
- PMID: 26508169
- PMCID: PMC4800173
- DOI: 10.1093/eurheartj/ehv512
Left ventricular heart failure and pulmonary hypertension
Abstract
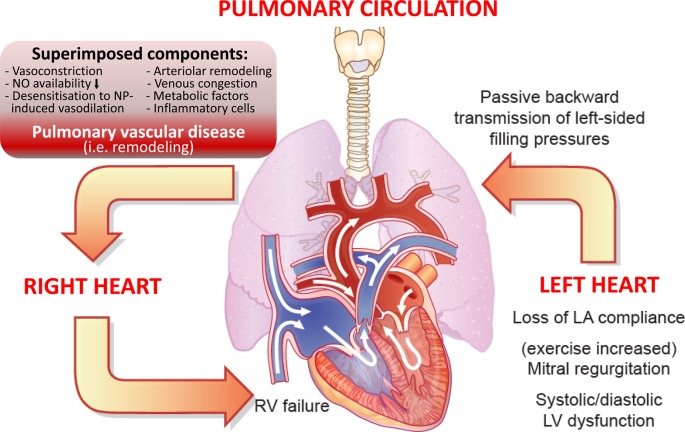
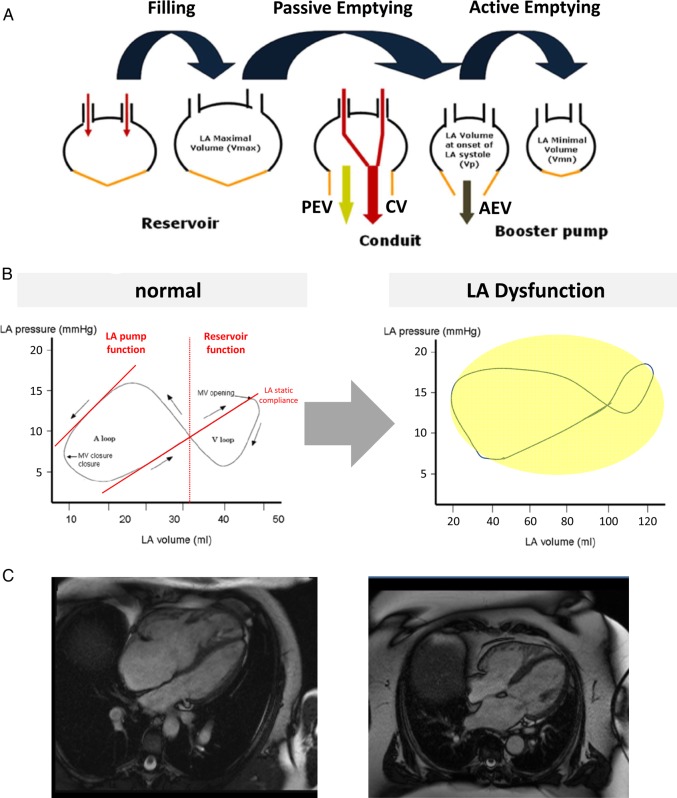
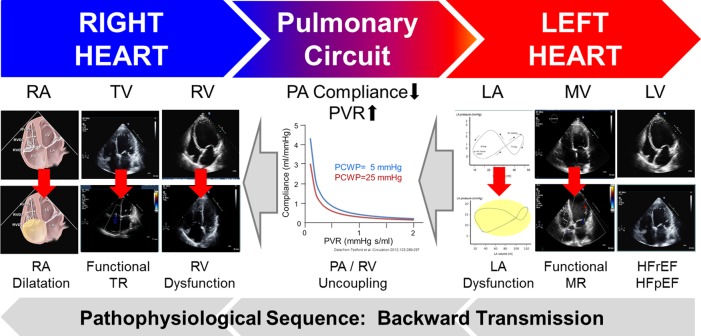
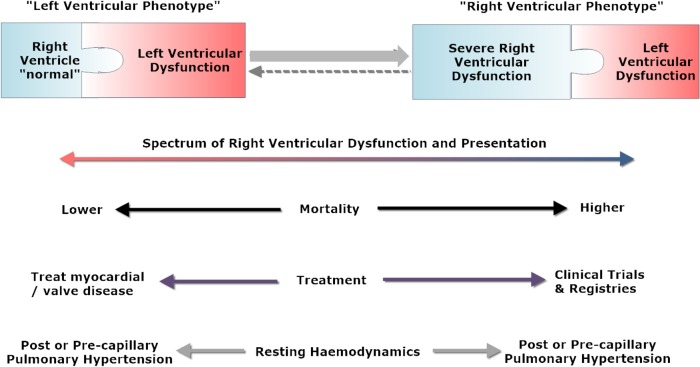
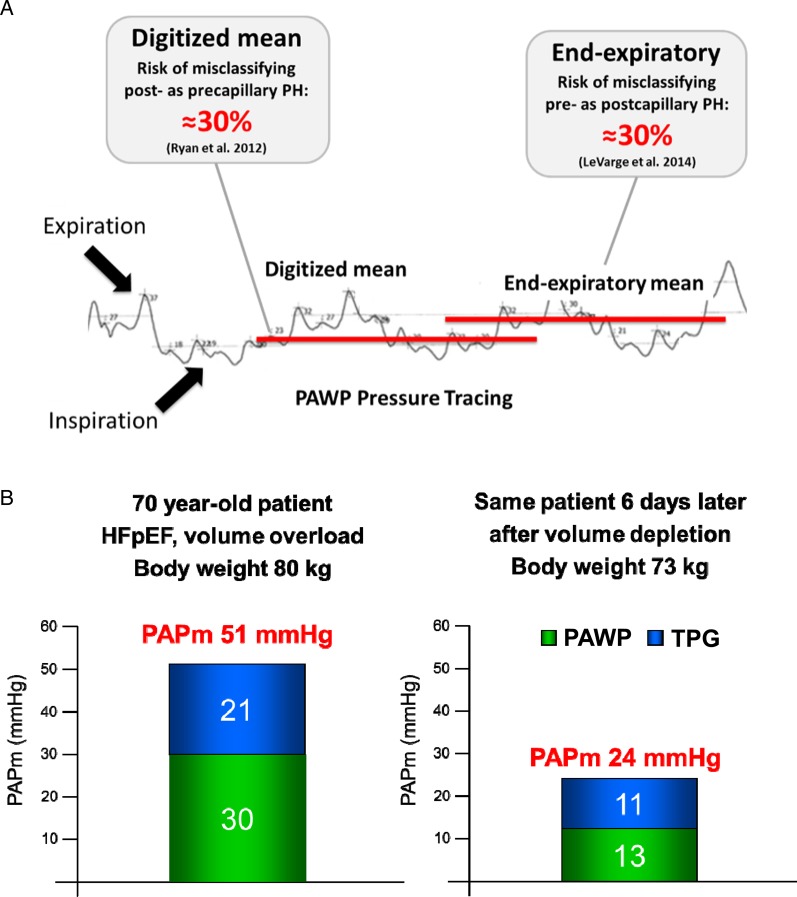
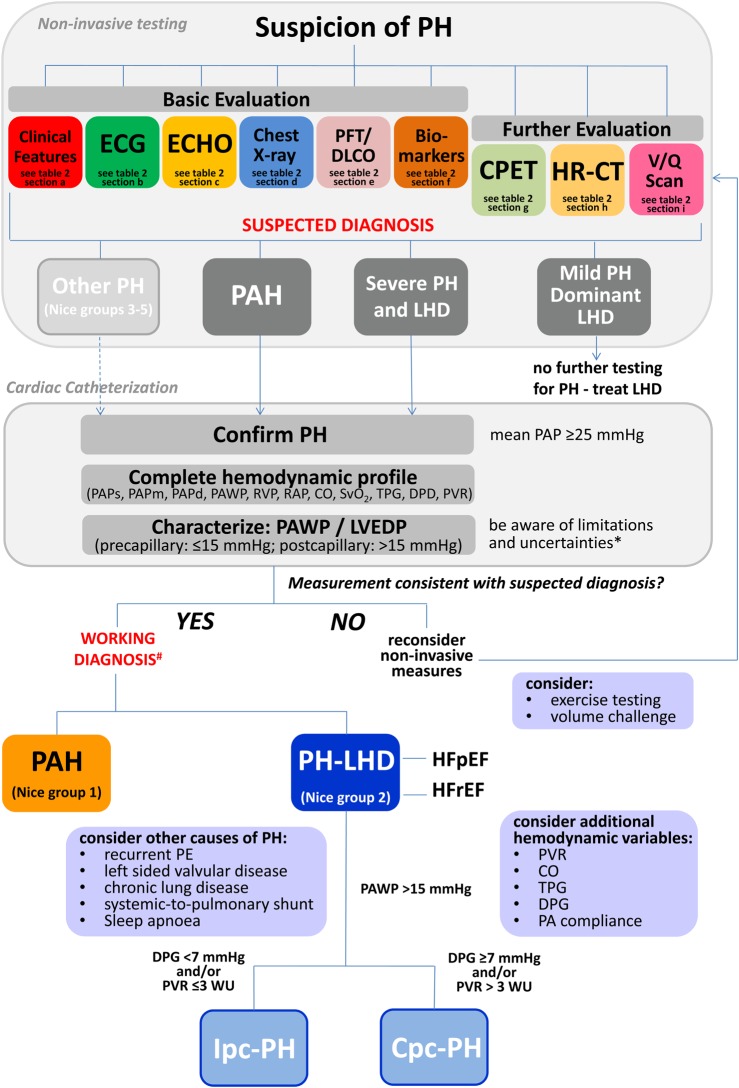
In patients with left ventricular heart failure (HF), the development of pulmonary hypertension (PH) and right ventricular (RV) dysfunction are frequent and have important impact on disease progression, morbidity, and mortality, and therefore warrant clinical attention. Pulmonary hypertension related to left heart disease (LHD) by far represents the most common form of PH, accounting for 65-80% of cases. The proper distinction between pulmonary arterial hypertension and PH-LHD may be challenging, yet it has direct therapeutic consequences. Despite recent advances in the pathophysiological understanding and clinical assessment, and adjustments in the haemodynamic definitions and classification of PH-LHD, the haemodynamic interrelations in combined post- and pre-capillary PH are complex, definitions and prognostic significance of haemodynamic variables characterizing the degree of pre-capillary PH in LHD remain suboptimal, and there are currently no evidence-based recommendations for the management of PH-LHD. Here, we highlight the prevalence and significance of PH and RV dysfunction in patients with both HF with reduced ejection fraction (HFrEF) and HF with preserved ejection fraction (HFpEF), and provide insights into the complex pathophysiology of cardiopulmonary interaction in LHD, which may lead to the evolution from a 'left ventricular phenotype' to a 'right ventricular phenotype' across the natural history of HF. Furthermore, we propose to better define the individual phenotype of PH by integrating the clinical context, non-invasive assessment, and invasive haemodynamic variables in a structured diagnostic work-up. Finally, we challenge current definitions and diagnostic short falls, and discuss gaps in evidence, therapeutic options and the necessity for future developments in this context.
Keywords: Heart failure; Post-capillary; Pre-capillary; Pulmonary hypertension.
© The Author 2015. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, Beghetti M, Corris P, Gaine S, Gibbs JS, Gomez-Sanchez MA, Jondeau G, Klepetko W, Opitz C, Peacock A, Rubin L, Zellweger M, Simonneau G; ESC Committee for Practice Guidelines (CPG). Guidelines for the diagnosis and treatment of pulmonary hypertension: The Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT). Eur Heart J 2009; 30: 2493–2537. - PubMed
-
- Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, Gomez Sanchez MA, Krishna Kumar R, Landzberg M, Machado RF, Olschewski H, Robbins IM, Souza R. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013; 62: D34–D41. - PubMed
-
- Rosenkranz S. Pulmonary hypertension 2015: Current definitions, terminology, and novel treatment options. Clin Res Cardiol 2015; 104: 197–207. - PubMed
-
- Galiè N, Corris PA, Frost A, Girgis RE, Granton J, Jing ZC, Klepetko W, McGoon MD, McLaughlin VV, Preston IR, Rubin LJ, Sandoval J, Seeger W, Keogh A. Updated treatment algorithm of pulmonary arterial hypertension. J Am Coll Cardiol 2013; 62(Suppl D): D60–D72. - PubMed
-
- Lüscher TF. Pulmonary embolism and pulmonary hypertension: Two issues often neglected in cardiology. Eur Heart J 2015; 36: 581–583. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
