

Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study
- PMID: 26509265
- PMCID: PMC4624940
- DOI: 10.1371/journal.pone.0140822
Assessment of Lower Limb Muscle Strength and Power Using Hand-Held and Fixed Dynamometry: A Reliability and Validity Study
Abstract
Introduction: Hand-held dynamometry (HHD) has never previously been used to examine isometric muscle power. Rate of force development (RFD) is often used for muscle power assessment, however no consensus currently exists on the most appropriate method of calculation. The aim of this study was to examine the reliability of different algorithms for RFD calculation and to examine the intra-rater, inter-rater, and inter-device reliability of HHD as well as the concurrent validity of HHD for the assessment of isometric lower limb muscle strength and power.
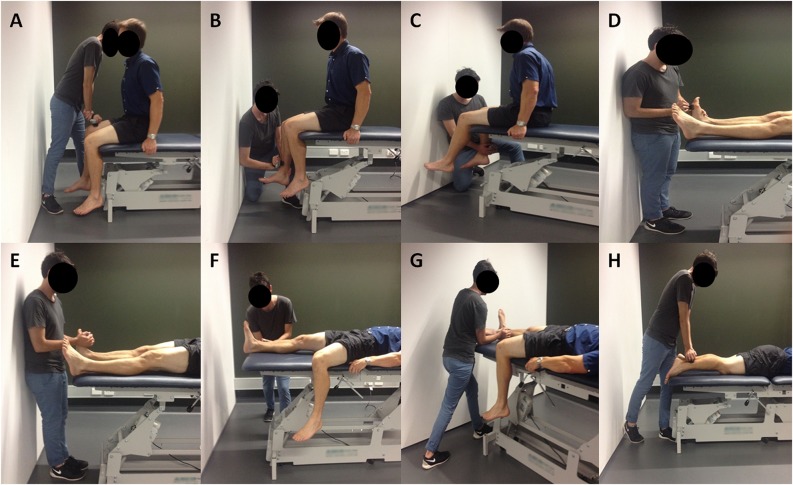
Methods: 30 healthy young adults (age: 23±5 yrs, male: 15) were assessed on two sessions. Isometric muscle strength and power were measured using peak force and RFD respectively using two HHDs (Lafayette Model-01165 and Hoggan microFET2) and a criterion-reference KinCom dynamometer. Statistical analysis of reliability and validity comprised intraclass correlation coefficients (ICC), Pearson correlations, concordance correlations, standard error of measurement, and minimal detectable change.
Results: Comparison of RFD methods revealed that a peak 200 ms moving window algorithm provided optimal reliability results. Intra-rater, inter-rater, and inter-device reliability analysis of peak force and RFD revealed mostly good to excellent reliability (coefficients ≥ 0.70) for all muscle groups. Concurrent validity analysis showed moderate to excellent relationships between HHD and fixed dynamometry for the hip and knee (ICCs ≥ 0.70) for both peak force and RFD, with mostly poor to good results shown for the ankle muscles (ICCs = 0.31-0.79).
Conclusions: Hand-held dynamometry has good to excellent reliability and validity for most measures of isometric lower limb strength and power in a healthy population, particularly for proximal muscle groups. To aid implementation we have created freely available software to extract these variables from data stored on the Lafayette device. Future research should examine the reliability and validity of these variables in clinical populations.
Conflict of interest statement
Figures
Similar articles
-
Intrarater reliability of hand held dynamometry in measuring lower extremity isometric strength using a portable stabilization device.Musculoskelet Sci Pract. 2017 Feb;27:137-141. doi: 10.1016/j.math.2016.07.010. Epub 2016 Jul 21. Musculoskelet Sci Pract. 2017. PMID: 27476066
-
Reliability and validity of the Performance Recorder 1 for measuring isometric knee flexor and extensor strength.Physiother Theory Pract. 2013 Nov;29(8):639-47. doi: 10.3109/09593985.2013.779337. Epub 2013 May 31. Physiother Theory Pract. 2013. PMID: 23724831 Clinical Trial.
-
Correlation of isokinetic and novel hand-held dynamometry measures of knee flexion and extension strength testing.J Sci Med Sport. 2012 Sep;15(5):444-50. doi: 10.1016/j.jsams.2012.01.003. Epub 2012 Mar 15. J Sci Med Sport. 2012. PMID: 22424705
-
Lower Extremity Handheld Dynamometry Strength Measurement in Children With Cerebral Palsy.Pediatr Phys Ther. 2016 Summer;28(2):136-53. doi: 10.1097/PEP.0000000000000228. Pediatr Phys Ther. 2016. PMID: 26744991 Review.
-
Muscle Strength and Power in People With Parkinson Disease: A Systematic Review and Meta-analysis.J Neurol Phys Ther. 2023 Jan 1;47(1):3-15. doi: 10.1097/NPT.0000000000000421. Epub 2022 Nov 1. J Neurol Phys Ther. 2023. PMID: 36318503
Cited by
-
The pilot study of the effect of six-week robot-assisted ankle training on mobility and strength of lower extremity and life habits for children with cerebral palsy.Heliyon. 2024 Jul 10;10(14):e34318. doi: 10.1016/j.heliyon.2024.e34318. eCollection 2024 Jul 30. Heliyon. 2024. PMID: 39114037 Free PMC article.
-
Effectiveness of proprioceptive training versus conventional exercises on postural sway in patients with early knee osteoarthritis - A randomized controlled trial protocol.Int J Surg Protoc. 2020 Sep 28;24:6-11. doi: 10.1016/j.isjp.2020.09.002. eCollection 2020. Int J Surg Protoc. 2020. PMID: 33089033 Free PMC article.
-
Effects of an urban forest healing program on cancer-related fatigue in cancer survivors.Support Care Cancer. 2023 Dec 5;32(1):4. doi: 10.1007/s00520-023-08214-3. Support Care Cancer. 2023. PMID: 38051396 Clinical Trial.
-
Investigating the Test-Retest Reliability and Validity of Hand-Held Dynamometry for Measuring Knee Strength in Older Women with Knee Osteoarthritis.Physiother Can. 2019 Summer;71(3):231-238. doi: 10.3138/ptc-2018-0051. Physiother Can. 2019. PMID: 31719719 Free PMC article.
-
Relative Validity and Reliability of Isometric Lower Extremity Strength Assessment in Older Adults by Using a Handheld Dynamometer.Sports Health. 2022 Nov-Dec;14(6):899-905. doi: 10.1177/19417381211063847. Epub 2022 Feb 4. Sports Health. 2022. PMID: 35120409 Free PMC article.
References
-
- Bohannon RW, Walsh S. Nature, reliability, and predictive value of muscle performance measures in patients with hemiparesis following stroke. Arch Phys Med Rehabil. 1992;73(8):721–5. - PubMed
-
- Doherty TJ. Invited review: aging and sarcopenia. J Appl Physiol. 2003;95(4):1717–27. - PubMed
-
- Wiley ME, Damiano DL. Lower-extremity strength profiles in spastic cerebral palsy. Dev Med Child Neurol. 1998;40(2):100–7. - PubMed
-
- Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol. 2002;93(4):1318–26. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
